The Importance of Healthy Bowel Movements
June 16 | Posted by mrossol | HealthA subject which seems to get the most time by parents with young children, and children with aging parents. mrossol
Source: The Importance of Healthy Bowel Movements
|
|
I believe one of the biggest issues in modern medicine is that patients often don’t get the opportunity to establish a genuine relationship with their physician and hence often lack the critical voice which is necessary for a therapeutic doctor-patient relationship.
Because of this, my goal here was always to be able to correspond with everyone who reached out to me (e.g., through comments or emails). Unfortunately, due to the unexpected success of this publication and the pressure it’s put on us produce content we feel is up to the standards the broader public deserves, I don’t have the time to both sufficiently correspond with readers and to publish biweekly articles. For that reason, I decided the best solution was to have monthly open threads where people could ask whatever they wanted on any topic and I would make a point to always reply to them.
In tandem with these open threads, I try to have them tie to a subject that I feel is important to cover, but didn’t quite fit as the focus of an entire article. For this month’s open thread, I want to focus on the importance of healthy bowel movements, some of the unnecessary challenges our society creates in this area, and the approaches we have used over the years to treat constipation.
Note: in the February’s open thread, I surveyed which future article topics had the most interest and I am presently finishing one for next week about ultraviolet blood irradiation since it was one of the most requested topics in that thread.
Missing Bowel Movements
Over the last month, I received a quite a few correspondences from readers asking me to write about constipation. This I believe is reflective of how widespread but rarely discussed constipation is, especially as one becomes older (where it often becomes one of the primary concerns of everyday life). Likewise, the primary diagnosis for constipation is “chronic idiopathic constipation” (CIC). Idiopathic, for reference means “no one knows why” which is remarkable given that existing studies find between 9-20% of adults (averaging at 14%) have CIC. This figure in turn varies greatly by country:
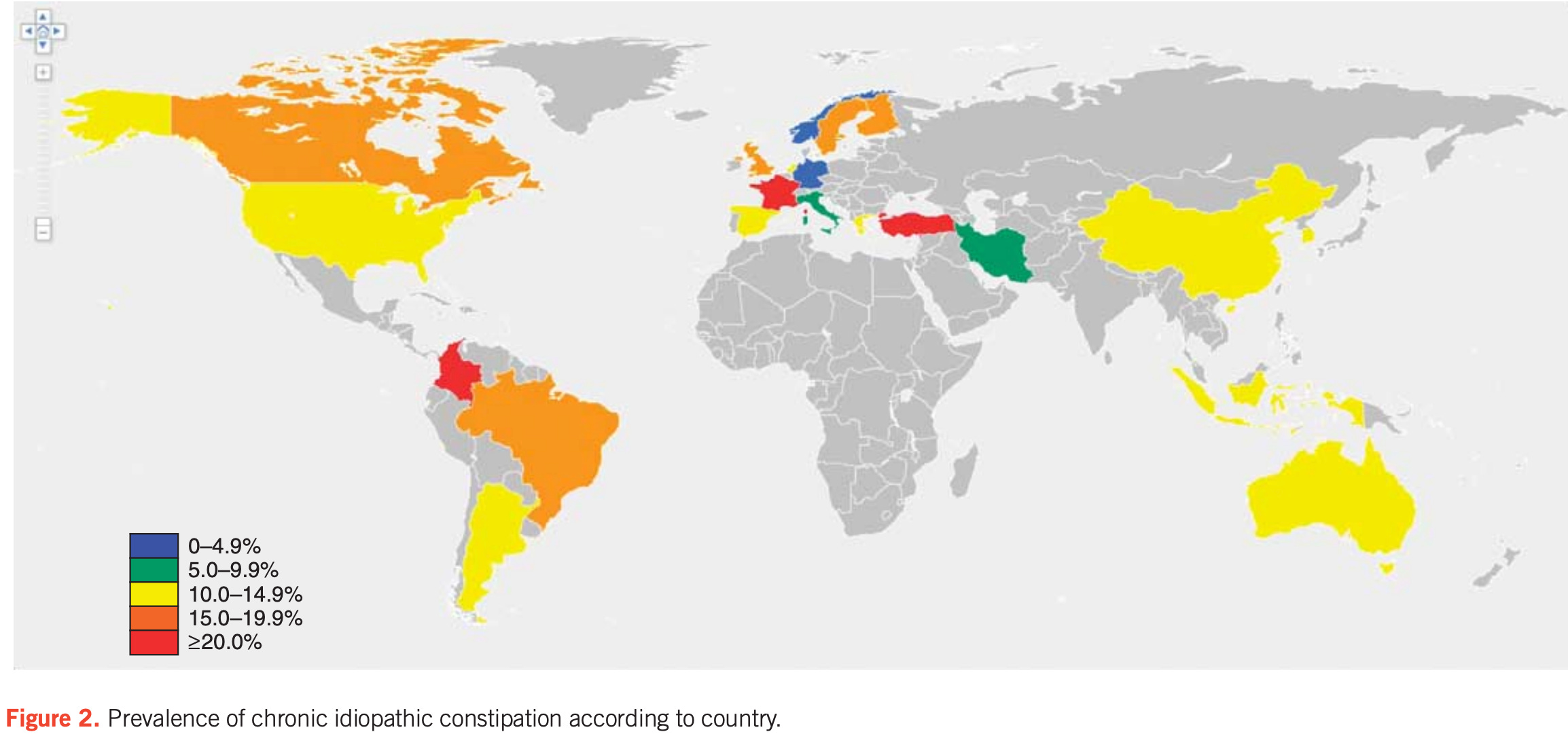 |
In tandem, there is no clear consensus on how to treat CIC (e.g., if you review the treatment guidelines, you will see they vary greatly depending on which country they were made in).
Likewise, the majority of patients do not even discuss their condition with their doctors:
Overall, 4,702 participants had experienced constipation (24.0% met the Rome IV CIC criteria). Among all respondents with previous constipation, 37.6% discussed their symptoms with a clinician (primary care provider 87.6%, gastroenterologist 26.0%, and urgent care/emergency room physician 7.7%).
We found that the locus of control—the extent to which individuals believe they can control events that affect them—is associated with constipation healthcare seeking. Namely, those with lower locus of control (i.e., believe symptoms are driven by others, chance, or fate) are more likely to consult with providers regarding their symptoms. However, individuals experiencing this maladaptive cognition may be resistant to both undergoing indicated diagnostic testing and accepting and adhering to treatments, thereby undercutting treatment success and reducing patient satisfaction.
Additionally, many who seek out medical help end up getting colonoscopy, a procedure which caries real risks and has no benefit here:
Among those who sought care, 54% reported previous diagnostic testing. Colonoscopy was the most commonly performed test; 46% of health seekers specifically underwent the procedure to evaluate their constipation. Although we did not ask the respondents about alarm features or have access to their medical records to confirm the “true” indication for the procedure, this suggests potential overuse of endoscopy in the evaluation of constipation. This is an issue because the diagnostic yield of colonoscopy for constipation is limited. Pepin and Ladabaum noted that in 234 individuals undergoing lower endoscopy solely for constipation, no cancers were found and only 3% had advanced lesions. The American Society for Gastrointestinal Endoscopy states that colonoscopy should not be performed in the initial evaluation of constipated patients without alarm features or suspicion of organic disease. The high usage of endoscopy and other tests seen in our study, in combination with the high prevalence of constipation, further reinforces the significant impact of constipation on population health and healthcare costs and emphasizes that efforts to reduce unnecessary testing are needed.
In short, there is a surprising gap of knowledge in this area, which I believe is best demonstrated by how many times I’ve been asked to admit a patient to a hospital who was essentially just severely constipated.
Note: the current research shows constipation hospitalizes 92,000 Americans each year and results in 1.3 million visits to American emergency rooms, which again illustrates our society’s lack of knowledge in this area, especially as the rate of this is increasing (e.g., from 2006 to 2011, there was a 42 percent rise in ER visits for constipation).
The Effects of Constipation
While it is relatively unlikely one will be hospitalized for constipation, the condition nonetheless has a significant effect on their quality of life as it is stressful to be unable to defecate when you attempt to and often quite uncomfortable once too much has built up inside you. Conversely, after a large bowel movement (especially if they’ve been constipated), individuals often feel much better and clear headed.
Note: I always wondered why the sense of well-being followed passing a large stool (especially a “toxic” one). Presently, I suspect Gerald Pollack’s model provides the answer. In it, he argues that the body is constantly forming a liquid crystalline water (H₃O₂) which is formed by eliminating protons from H₂O, and that this fourth phase of water makes much of life possible (e.g., it’s responsible for the structural integrity of the body and generating the flow of fluids through the body). This process however creates a large number of protons the body must excrete to maintain its negative charge, which Pollack argues occurs through the breath, sweat, feces and urine. I, in turn, suspect that the rapid sense of well being individuals feel after certain bowel movements is a result of the electrical charge gradient of the body normalizing, as many of the descriptions I’ve heard match what happens when there is an improvement of the physiologic zeta potential(which likewise comes from increasing the net negative charge of the body).
Furthermore, constipation frequently results in a variety of significant issues. Most commonly, we recognize its connection to the fact the pressure created by strained bowel movements can lead to haemorrhoids, rectal prolapse, and anal fissures (all of in turn which make bowel movements much more challenging).
However, it also can lead to a variety of less appreciated issues. These include:
•Dysbiosis within the gut microbiome (and the variety of complex issues which can accompany it). In many cases, the gut dysbiosis which leads to constipation results from the foods you digest not being fully digested (which for example is why it is important to chew your food and have a sufficiently acidic stomach).
Note: one of the most interesting things I learned in this area is that SIBO(one of the more challenging gut dysbioses) often results from slowed bowel transit time, and in turn, the practitioners who I find are the most successful with treating SIBO focus on increasing peristalsis.
•Fatigue (e.g., consider this study in the elderly), headaches, abdominal pain, nausea, and vomiting.
•Chronic constipation being linked to a variety of progressively more severe illnesses including diverticulitis, kidney disease, gastric and colorectal cancer, ischemic colitis, and Parkinson’s disease.
Note: certain chronic illnesses (e.g., multiple sclerosis) can cause constipation (e.g., MS does it by interfering with the normal function of nerves within the body) which is unfortunate as constipation and a dysfunctional microbiome increases one’s risk for these degenerative conditions.
The Causes of Constipation.
Since most constipation is labeled as “idiopathic” treatments to constipation are typically symptom based (which many are happy to do for the rest of their lives given how challenging constipation is to deal with). Unfortunately, while laxatives are relatively benign if used occasionally, over time, they can impair the normal function of the GI tract (e.g., they can alter the gut microbiome) and hence create a situation where one requires chronic laxative use.
Note: Dr. Hazan, an expert in this area, has also seen instances where laxatives destroyed the normal functioning of the colon which then required part of the colon to be surgically removed.
Additionally, we find one of the most commonly used laxatives (MiraLAX) can create issues because a surprising number of people have sensitivities or allergies to polyethylene glycol (e.g., I know people who were unaware they had the allergy and then had anaphylaxis after they took it as preparation for a colonoscopy along with patients who developed neurological complication from it). Furthermore, when individuals have a delayed bowel transit time (e.g., anyone who is constipated), individuals are more likely to systemically absorb MiraLAX and experience toxicity from it.
Note: one of the major concerns with the COVID vaccines was that fact the lipid nanoparticles contained within it had polyethylene glycol (PEG) and hence would affect those within the population who had an undiagnosed allergy to it. Sadly, because vaccines are 100% safe and effective, even people I know who had documented anaphylactic PEG allergies predating COVID-19 were not given exemptions from COVID vaccination (and neither were those who had documented anaphylactic reactions to the first shot).
When evaluating constipation, it’s important to consider the presence of a co-existing medical diagnosis. For example, three important conditions to be aware of if you have chronic and unusual constipation (that are easy to test for) are as follows:
•Colon Cancer. When a tumor grows in the colon, it progressively blocks transit through the colon, which in turn leads to the feces which get through becoming narrower and narrower (along with abnormal weight loss, anemia and rectal bleeding). Because of this, if you notice that gradually happening to you, it is worth getting a preliminary test to see if you made have a cancer (there are simple and complex ways to test the stools for colon cancer).
Note: red meat (especially for those who do not eat it frequently) and beet juice (which also reddens the urine) can make both the stools turn red. Because of this, I’ve had numerous panicked people contact me over the years about rectal “bleeding” they thought was a cancer which in reality was due to drinking beet juice.
•Hypothyroidism. One of the common symptoms of hypothyroidism (beyond hair loss, coldness, fatigue, and weight gain) is delayed bowel transit time.
•Hyperparathyroidism. This is a surprisingly common but unrecognized condition which can make individuals feel quite ill (e.g., it can cause pain throughout the body, cognitive issues, arrhythmias, kidney stones, unexpected fractures and a variety of gastro intestinal issues).
Note: endometriosis can also sometimes cause constipation. Likewise, a variety of neurological disorders can affect the normal motility of the gastrointestinal tract .
In most cases however, the cause of constipation remains unknown (e.g., outside of opioid induced constipation, providers rarely evaluate if a pharmaceutical drug is contributing to it) and typically the advice given is to “eat more fiber,” which while sometimes helpful, can often be problematic if the issue is a lack of motility (movement) within the digestive tract.
Note: many other pharmaceutical drugs besides opioids can also cause constipation (e.g., antacids, anticholinergics [such as those taken for incontinence] antidepressants, antihistamines, antipsychotics, calcium channel blockers, certain blood pressure medications, and NSAIDs). Because of this, if you develop constipation after starting a new prescription, it is always important to see if that drug is linked to impaired bowel movements. Additionally, iron and calcium supplements can sometimes cause constipation.
Presently, I believe there are a few major contributors to the epidemic of constipation we face that are largely overlooked. They are as follows:
•Poor diet. For example, one of the world’s leading experts on holistic gastroenterology has found apples, bananas, chocolate, rice and white bread to be some of the most common dietary causes of constipation. In my own experience, certain foods (such as those ones) frequently contribute to chronic constipation, and it is thus important to compare your diet to your subsequent bowel movements to determine which foods make you constipated.
Note: within Chinese medicine, they have an entire diagnostic model based on looking at the characteristics of one’s stools. While this is largely avoided in our society (due to the disgust it will often illicit), I have often found it to be extremely useful, and I often monitor my own stools to assess how my body is handling my current diet (or how long it takes a food to transit my GI tract). Likewise, I have had many patients who found the Chinese medicine approach to treating constipation quite helpful for them.
•A disrupted gut microbiome (which conversely becomes disrupted by bowel stasis).
•Mineral deficiencies (primarily magnesium and in some cases potassium).
•Dysfunction within the autonomic nervous system (which amongst other things is a common consequence of many of the constipation triggering drugs I listed previously).
•Chronic dehydration or an impaired zeta potential (e.g., I’ve seen numerous cases of the bowels coming back to life after a patient’s zeta potential was improved).
•Individuals not allowing themselves the time to go to the bathroom when they need to defecate as once they miss this window, they often subsequently cannot.
Note: within Chinese medicine, it is believed that different organs activate at certain times in the day. In that system, the colon activates between 5-7 AM, and I’ve had numerous patients who have found if they do not use that time to have a bowel movement at that time, it’s often quite difficult to for the rest of the day. While the time varies from person to person, I believe it is important to prioritize listening to the defecation signals your body gives you and not putting off going to the toilet.
•Our sedentary lifestyles reducing the inherent motion within the gastrointestinal tract.
•The position we go to the toilet on.
Squatting
Something many people don’t realize is that the modern toilet is a relatively new invention, and that prior to it, rather than sitting, humans squatted to go to the bathroom. Additionally, sitting toilets are primarily a Western creation, so as one goes to many other societies, squatting toiles are much more common (although they are gradually being phased out as a sitting toilet is seen as a sign of affluence).
Note: the full history of toilets can be found here.
For example, toilets like these are commonly seen throughout Asia.
 |
Note: one of the interesting things about this design is how much less water it uses (whereas by contrast, standard toilets account for approximately 30%of the average home’s indoor water use).
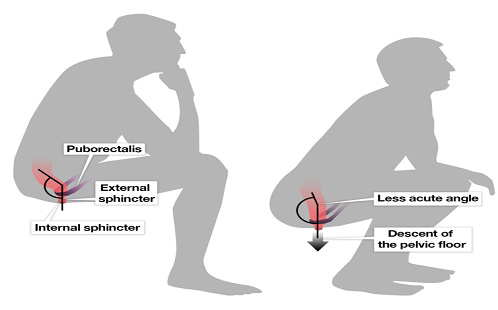
Unfortunately, due to our anatomy, this positional change is much more problematic than we realize as it compresses the rectum and hence makes it much harder to force feces through it.
 |
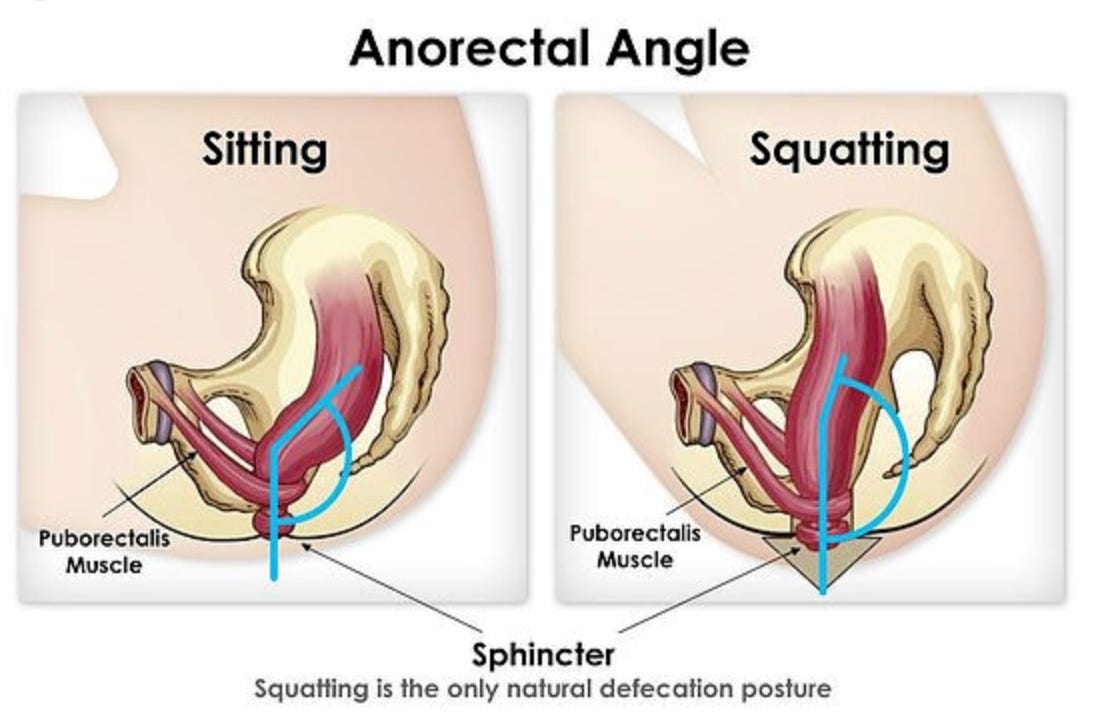 |
In turn, many find that if they squat while defecating, they have a dramatically easier time going to the bathroom (e.g., I periodically hear this story from patients who went to Asia and had to use squat toilets there). Sadly, however, like many other harmful modern cultural practices (e.g., there are a variety of issues with wearing bras), the importance of this is rarely recognized.
Treatments for Constipation
Given how common constipation is and how many different approaches exist for treating it, it often falls to the individual to determine which approach helps them the most (e.g., many people find prune juice is very helpful for them). In the final part of this month’s open thread, I will share some of the non-standard approaches we have found to be the most useful for treating constipation. Likewise, if you have an approach that worked for you, please share it, but remember that the primary function of this thread is to be able to enquire about any topic you wish to ask about about…

Unlock this post for free, courtesy of A Midwestern Doctor.
| Claim my free post |




Leave a Reply
You must be logged in to post a comment.