GRACESCHARA.COM LAWSUIT UPDATES
November 4 | Posted by mrossol | Law, Losing Freedom, MedicineMy friend Scott Schara is still fighting the corrupt system that defeated him in superior court. He has now lost two children, the first to hospital murder, and the latest to suicide.
Source: 389. Midweek repost: GRACESCHARA.COM LAWSUIT UPDATES
|
|
Yoho note
If you have not kept up with this case, the following may be confusing. Here are a few notes to help you:
- Grace, Scott’s daughter with Down Syndrome, was killed by a combination of sedatives administered by medical personnel. This was clearly malpractice. I know; I am an expert in sedation from a long career of using these drugs in surgery.
- Dr. Berdine was the plaintiff’s witness, and for some odd reason, the judge permitted multiple defense witnesses.
- The federal incentives to the hospital to murder patients with Covid run into the hundreds of thousands of dollars. There are separate financial rewards for intubation (putting a tube in the trachea to facilitate respiration) and death. Yes, this is hard to believe.
- Grace had no medical indication for any of this “treatment.” She was alert and speaking before the doctors decided it was time to slaughter her.
- Obtaining justice from a court requires a mammoth investment of time and money, but in this case, the hospital killed the wrong person.
- Juries are easily fooled with enough lawyering, particularly if the judge is complicit with one side, as seemed to be the case here.
- Scenarios like this still happen every day across America. Families seldom understand what is happening. They are paid to stay quiet anyway, with $10,000 in funeral expenses.
- I came from an old school where patient welfare was our only priority. How hospital medicine could have devolved to this stuns me every time I consider it.
Motion for New Trial Filed in the Only COVID Wrongful Death Case to go to a Jury
Landmark lawsuit
NOV 03, 2025
Before explaining the Motion, Grace is the reason for jumping into this fight. I don’t want my worst enemies to lose their best buddies to a system that is under government control.
 |
 |
The verdict on June 19 was in favor of the medical industrial establishment. Did the jury get it wrong? Juries get things wrong every day.
The defense, through their “experts,” said that by being in a hospital, you are giving implied consent, and that the drugs that euthanized Grace were normal in an ICU, so no informed consent is necessary. Doctors informing the family is not even necessary for the two prior overdoses; the third overdose is what killed Grace. Finally, their experts stated that a DNI (Do Not Intubate) = DNR (Do Not Resuscitate), and a doctor can unilaterally place a DNR on a patient, without consent, without a witness, without a signature, and without a DNR bracelet. The jury sided with the defense. My wife, our daughter Jessica, and I had legal power of attorney, which is an invention in their legal system, but this didn’t matter to the jury.
Last week, I filed a motion for a new trial. The motion rebukes the injustice of the court.
 |
The entire motion can be reviewed below:
 |
New Trial Motion
In short, I believe that newly discovered evidence showed Judge McGinnis’s personal bias.
Specifically, the judge denied all of our Motions in Limine (MIL) without discussion.
A motion in limine is a pretrial motion in the U.S. legal system, derived from the Latin phrase meaning “at the start” or “on the threshold,” filed to request that certain testimony or evidence be excluded from trial before it is presented to the jury. These motions are typically discussed outside the presence of the jury and are used to prevent the introduction of evidence that is irrelevant, inadmissible, unfairly prejudicial, or potentially harmful to a fair trial. The primary purpose is to avoid the jury being tainted by information they cannot unhear, even if an objection is later sustained.
The motion requests a new trial based on the denial of the MIL. The following are clips from the Motion, organized by subheading.
 |
From pp. 1-2:
 |
From pp. 6-7:
 |
 |
From pp. 7-9:
 |
 |
From pp. 16-17 and 29-30:
 |
 |
 |
From p. 25:
 |
 |
 |
From p. 28 and 31:
 |
 |
 |
Today, I want to get back into the nefarious details surrounding her death. I would like to take this opportunity to reflect on her last day on earth and then tie together the Motion filed last week with these facts.
Before I begin, please take 10 minutes to read this article published by The New American on October 11, after the reporter conducted post-trial research on the case.
 |
For a larger perspective, please take a moment to review the timeline below. We presented this timeline to the jury during Grace’s trial. Online viewers could not see this timeline because it was on the court’s television screen, outside of the camera view.
 |
Already at midnight, the nursing staff was increasing Precedex. By 7:00 a.m., this drug was at or above the rate that caused two prior overdose events.
The previous evening, October 12, Jess was with Grace, and she Facetimed Cindy and me, as well as her nephews. She easily proned with oxygen saturations at 98/99% on a lower dosage of Precedex. Why the increase?
Bigger picture, during the 48 hours Grace was denied advocacy (in total), the nursing staff increased the dosage of Precedex seven times – all after her known reaction to Precedex, which caused two prior overdose events. It is unconscionable for someone with Down Syndrome to be without an advocate, especially in a hospital.
The Precedex Package Insert, being admitted into evidence, was one of the many items that showed the patient was ignored in favor of the diagnosis. When Precedex was shut off on October 9, Grace was herself and had a great day. After I was “escorted” out of the hospital on October 10, Precedex was started back up. At midnight on October 13, the first entry in the timeline above, Grace had already been on Precedex continuously for 52 hours.
These medical records demonstrate that Grace was chemically restrainedbefore her death on October 13.
 |
 |
 |
 |
At 10:48 a.m., Precedex was “officially” increased to the maximum allowable dosage.
 |
The nursing notes, supported by deposition testimony, show this increase to the maximum allowable dosage actually happened at 8:40 a.m.
 |
 |
 |
At 8:40 a.m., Grace was at a rate 40% higher than the dosages that caused two prior overdose events. These prior events were ignored.
From Dr. Berdine’s (our medical expert) deposition, relative to Precedex:
 |
What is interesting about the timing is that the dosage was increased to the maximum during the hour that Jess was told she needed to go home and take a shower. Nurse McInnis told Jess she had to leave to take a shower because of her supposed belief that the “virus” was aerosolized, and Jess would not be protected due to not being able to wear PPE in the shower. Grace was in a negative-pressure room. She was also outside the window of having COVID, according to one of their gods – the CDC.
During that short window of time while Jess was gone, Grace wanted to get out of bed to use the bathroom. Instead, she was strapped down to the bed and given the maximum dosage of Precedex.
During her testimony, Nurse McInnis stated that Grace was never in physical restraints; however, she said Grace was placed in mitts after the feeding tube was inserted to prevent her from pulling on it. Jess testified that mitts were not used during the feeding tube process, and Grace was in restraints when she got back shortly after 9:00 a.m., after going home to take a shower. Nurse McInnis was Grace’s only patient, which means she put Grace in restraints.
 |
Dr. Shokar’s progress note confirms Jess’s testimony.
 |
Strangely, there was no order for the restraints! Why not?
Consistent with the “inconsistencies” at the trial and in the medical records, take a look at this next record. Interestingly, it was not part of the medical records received in my records request, but was given to the defense by the hospital.
St. Elizabeth’s Hospital did not report Grace being in restraints to the Department of Health Services. Why not?
 |
 |
I want to move on to the illegal DNR order.
Dr. Shokar entered a DNR order simultaneously at the end of the call with me and Cindy at 10:56 a.m. on October 13. Why didn’t he simply say, “Since you decided you don’t want to give us a preauthorization to intubate Grace, I’m going to enter her as DNR on her medical chart.” That simple communication would have made the difference between life and death. Instead, he presented a hypothetical of having to keep working on Grace over and over in the event of her heart stopping AFTER getting us to approve a feeding tube because “Grace had such a good day yesterday that we should work on nutrition.” We were unaware of the DNR order until it was too late. As we learned at the trial, Nurse McInnis “forgot” to put the purple DNR bracelet on Grace. That would have been an alarm bell that would have facilitated us immediately removing the DNR order from Grace’s record. Think about how fast Jess would have called us if a DNR bracelet had been put on Grace.
 |
Since the COVID PSYOP, many studies have been done. Here’s a not-so-surprising research article regarding the use of DNR orders on patients with Down Syndrome:
 |
The article explained that from January 2019 – June 2022, if the patient had Down Syndrome, he/she was 630% more likely to have a DNR status ordered by the hospital. This statistic is a result of a review of records from 825 hospitals representing 1,739,549 patients with COVID. I was quoting from this article when asked the question regarding my perspective. The defense objected, and the judge sustained the objection. Now you know the truth.
Cindy and I approved the feeding tube during the call, which started at 10:12 a.m. Dr. Shokar told us Grace had such a good day on the 12th that we should work on nutrition and get her moving so she can get out of the hospital in the next several days. We were not surprised based on what Jess had told us about Grace’s oxygen level overnight.
The approval of a feeding tube facilitated the kiss of death. Nurse McInnis justified the feeding tube even though she described Grace as “near death.”
 |
Nurse McInnis combined Lorazepam (at 11:25 a.m.) with the already overdosed Precedex – unilaterally. The reason given at trial was that Lorazepam was necessary to control expected anxiety related to the feeding tube. Why didn’t Dr. Shokar mention Lorazepam during the “informed consent” discussion regarding the feeding tube? Grace was already on maximum sedation with Precedex – think about this for a moment. More importantly, Jess was there to comfort Grace, but was kept away from the bed by Nurse McInnis.
Nurse McInnis gave Grace two more doses of Lorazepam at 5:46 p.m. and 5:49 p.m., even though she charted Grace as “somnolent min/no response.” Grace was now at a dosage of Lorazepam 50% higher than she had ever been during her brief hospital stay. Lorazepam has a 12 – 14-hour half-life.
Dr. Shokar ordered, and Nurse McInnis gave Grace morphine at 6:15 p.m. morphine Package Insert warnings are plain to see for anyone who wants to put patient care above hospital protocols. He also ordered her to shut off Precedex before giving Grace morphine.
 |
Dr. Berdine testified that the combination of drugs Grace was given has a synergistic effect.
 |
Additionally, Grace did not have a detectable blood pressure at this time, according to Nurse McInnis’s own record at 6:09 p.m.
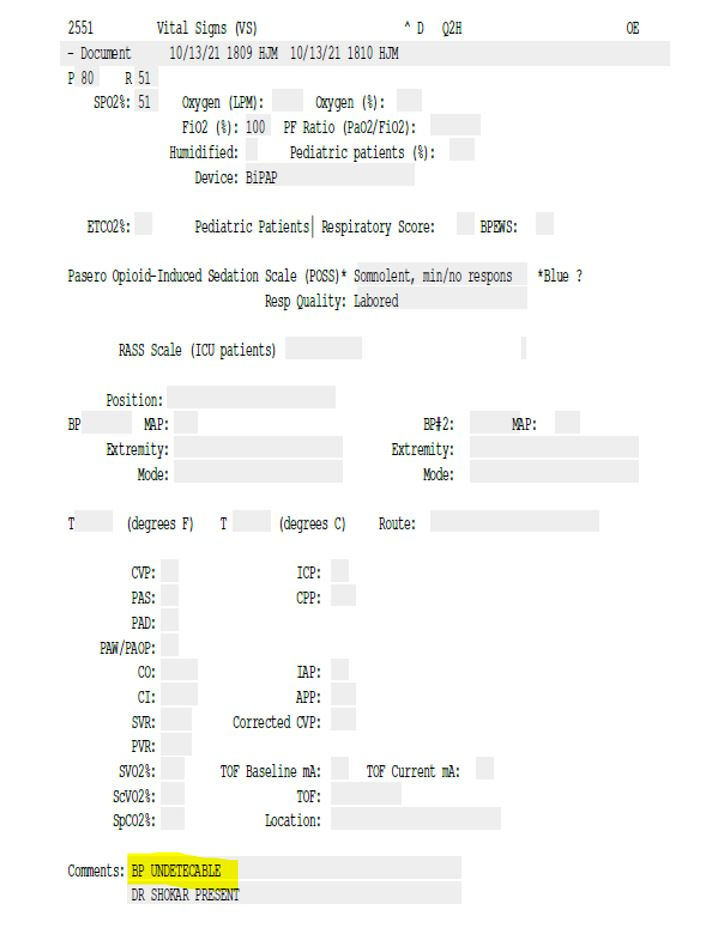 |
This fact led to Dr. Berdine’s testimony that giving Grace morphine was the worst clinical decision he has ever seen in over 46 years of medical practice. Dr. Berdine’s case summary is posted on YouTube.
 |
A responsible doctor and nurse are to be closely monitoring the patient and have the reversal drug immediately available. Neither happened. According to her trial testimony, Nurse McInnis left promptly at 7:00 p.m. [Her timecard, the length of the courtroom away from her station, showed she punched out at 7:36 p.m., nine minutes after Grace died – she testified that she didn’t know Grace died until the next day.] Jess’s testimony stated that Nurse McInnis would not come into the room when Jess felt Grace getting cold, but instead told Jess ‘That’s normal, just cover her with a blanket.’ Furthermore, Jess testified that Nurse McInnis told her, ‘we’ve done everything we can for your sister’ – after 7:00 p.m. Dr. Shokar’s shift ended at 6:00 p.m. He was in Grace’s room until approximately 6:30 p.m. He called me at 6:43 p.m. to inform me that ‘Grace had another good day and he just gave her morphine to slow her breathing down.’
Was the Precedex shut off before the morphine, as Dr. Shokar ordered?
During the trial, one of the most notable testimonies was that Precedex was shut off before the morphine injection, contradicting the medical record. Dr. Shokar stated that he didn’t believe the medical record. Their nurse expert, Julie Davis, testified that the recording of entries is often late and noted in the records that way. Interestingly, the culprit is again Nurse McInnis. Look at how she recorded the 6:15 p.m. morphine injection, at 6:30 p.m. – the late entry is noted with parentheses:
 |
Now look at how she recorded the Precedex being turned off at 6:37 p.m.:
 |
The morphine and Precedex entries were recorded within 7 minutes of each other. There was no late recording notation for Precedex. The jury saw another anomaly but decided to look the other way, siding again with Goliath.
Finally, what about the nurses standing around, claiming Grace was DNR, refusing to do anything after we screamed that Grace was not DNR? Dr. Berdine testified that Naloxone should have been given to reverse the morphine, and the reversal agent for Lorazepam should also have been given. In Dr. Shokar’s deposition, he acknowledged that reversal drugs should not be ignored because of code status:
 |
 |
The defense knew of everything I presented in this report (other than the article regarding Down Syndrome patients and DNRs), and this was only Grace’s last day. What did they do with these facts?
They hired six experts to uniformly testify that the treatment of Grace met the Standard of Care AND that Informed Consent is not necessary in an ICU. Even further, they claimed (and the jury agreed) that when you enter a hospital, you are giving implied consent to their protocols. The experts for the defense presented a case that had nothing to do with the medications that killed Grace or the illegal DNR order. Of course, that was their job.
As we know, protocols can kill people.
Dr. Berdine’s testimony regarding Informed Consent and the Standard of Care was 180 degrees different. He was the most credible expert at the trial.
Even more important, because of the denial of the MIL, the defense was allowed to attack our family’s religious beliefs and beliefs about the medical system developed after Grace died. From pp. 9-10 of the Motion:
 |
I believe the jury could have gotten it right if it were not for the denial of the MIL. Denial of the MIL facilitated the defense being able to paint me as an outsider – a conspiracy theorist. Again, this is what they were paid to do.
We’ve been programmed to believe the legal system is a justice system. Hopefully, more are waking up to the anti-Christ systems that are being used to control the world.
Here’s what God has to say about the courtroom:
 |
 |
We appreciate the ongoing support, encouragement, and prayers. May God bless each of you.
 |
 |
Grace’s Dad
Scott Schara, President
Our Amazing Grace ™
 |
1 Sam 17:47
Our Amazing Grace is a trademark of Our Amazing Grace’s Light Shines On, Inc.
Discussion about this post
I am so happy to see your persistent and positive challenge to the audacious authoritarianism of the destructive forces in our medical system. I dare not call it “healthcare” as there is nothing healthy or caring about it; corporatized medical management is about the kindest thing it can be called. Mistakes were not made; crimes were committed. And they continue and ever shall unless we demand better. Thank you, Schara family, for going many extra miles to right these wrongs. I continue to pray for your resounding success!
Grace Got Covid; Grace Died of Covid; Get Over It!
 |
 |
You’re a free subscriber to Surviving Healthcare. This post is public, so feel free to share it.




Leave a Reply
You must be logged in to post a comment.