Why Have Vaccines Become a Religion?
November 17 | Posted by mrossol | CDC NIH, FDA, Pharma, Transparency[non], VaccineEvery parent should be required to read this. Belief in vaccines is just that, a BELIEF. The ‘science’ is sketchy, at best. mrossol
Source: Why Have Vaccines Become a Religion?
|
|
As more and more people are awakening to the dangers of vaccines, they are gradually discovering a problem vaccine safety advocates have had to deal with for decades—talking to vaccine zealots is like speaking to a brick wall and regardless of the evidence you put forward, can’t reach them (sometimes seeming as though you are speaking to a religious fanatic who is unwilling to even consider the “blasphemy you are spewing forth”).
For example, in 2009 after nephrologist Dr. Suzanne Humphries noticed patients (particularly hospitalized ones) kept on developing kidney failure after flu shots, she experienced significant pushback from trying to delay vaccinating until discharge:
In the past when I was consulted on kidney failure cases and said, “Oh that was the statin/antibiotic/diuretic that did that!” instantly the drug would be stopped—no questions asked. Now, however, a new standard was applied to vaccines. It didn’t matter that the internist’s notes in the charts said, “No obvious etiology of kidney failure found after thorough evaluation.”
The next time the medical chief of staff and I met in the corridor, an oncologist was present. At one point, I asked the chief, “Why doesn’t anyone else see the problem here? Why is it just me? How can you think all this is okay? Why is it now considered normal to vaccinate very sick people on their first hospital day?” The oncologist gave an answer that surprised me. She said, “Medical religion!” and turned and walked away.
Several months went by, and the medical executive committee met to discuss my concerns, without allowing me to be present at the meeting. I was informed in writing that the nursing staff were becoming confused by me discontinuing orders to vaccinate and that I should adhere to hospital policy. I thought this odd, given that nurses are not accustomed to giving the same treatment to every patient, and are fully capable of reading individualized orders.
As time went on, it was interesting seeing the divide in the hospital staff. Nurses would bail me up in quiet corners and tell me stories that completely backed up what I was seeing. They would guardedly support me, when their superiors were out of eye- or ear-shot.
I wrote all the cases out and put together a comprehensive brief for the hospital administration, but to no avail. Not even science could get through as the snake-oil salesmen continued to deny my findings.
I kept presenting the administration with facts they could not respond to, in the hope that they would get a blinding revelation of the obvious. Finally, they recruited the Northeast Healthcare Quality Foundation, the “quality improvement organization” for Maine, New Hampshire and Vermont, to get me off their backs. Dr. Lawrence D. Ramunno sent a letter invoking the fallacy of authority, which adamantly informed me that hospital vaccination against influenza virus would become a global measure for all admissions in 2010 [due to Obamacare], and that my evidence of harm was not significant because 10 professional organizations endorse vaccination.
This condescending, vapid letter…illustrated callous disregard of clinicians at the highest level, and the willful blindness prepared to ignore clearly documented cases, and their own medical literature. Not satisfied with demanding that I practice automaton obedience to dictates from on high, they initiated a shadow observation, where everything I did and wrote in the hospital, from then on, was observed and scrutinized.
Note: prior to Obamacare effectively mandating flu shots for healthcare workers, many doctors I knew did not vaccinate as they felt there were negligible benefits to the shot and real potential risks and thought the new mandate didn’t make sense. I do not believe my sample was biased as other sources corroborated it (e.g., this 2009 CNN segment discussed New York healthcare workers protesting a state law requiring annual flu shots for them)—making it remarkable how quickly a simple mandate was able to shift critical thinking on this topic to an irrational embrace of vaccination (especially given how people I’ve met who got Guillain-Barré syndrome from a vaccine).
Worse still, decades of propaganda have enshrined a number of ridiculous standards and rationalizations to defend vaccines you are always expected to argue against if you so much as question them.
Note: propaganda is a tool that is used to convince the population that something which goes against their interests and cannot be logically justified is actually “good for them.” For this reason, propaganda is emotional rather than logical in nature, and frequently will use emotional arguments that on the surface appear logical but once you peer deeper are not.
Why Do People Believe in Vaccines?
Once people awaken to the vaccine issues, one of the most frequent questions which emerges is why the medical field has such a rigid ideological attachment to them. I would argue it is due to three interrelated reasons:
First, human society has always been defined by competing groups vying for status and wealth, and what many do not appreciate is that, historically, it is a very recent development that doctors attracted the prestige and salary the profession commands. This I would argue was ultimately a result of two things:
•Market monopolization (via the American Medical Association) and technological developments birthing an incredibly profitable medical industry, which generated the funding to market a newfound faith in it to the entire country and required doctors (and faith in doctors) to serve as the keystone for the industry.
•Medicine creating a mythology that it rescued us from the dark ages of disease, and hence deserves its supremacy in the current social hierarchy. As “vaccines ending infectious diseases” is a central part of that mythology, to maintain their existing prestige, those within the conventional medical system are essentially forced to double-down on the absolute supremacy of vaccines, regardless of the evidence against them, or the fact, as Secretary Kennedy brilliantly shows here, there is no actual evidence vaccines were responsible for the decline in infectious disease the medical industry falsely claimed credit for.
Note: when Dr. Humphries raised her concerns about influenza vaccines causing kidney failure, colleagues used the mythology of medicine’s most esteemed vaccines to dismiss her (e.g., “[the chief of internal medicine] went on to remind me that ‘smallpox was eradicated by vaccines, and polio was eradicated in the United States by vaccines.’”). This eventually motivated Humphries to scrutinize that mythology and create the pivotal book Dissolving Illusions that showed exactly why that mythology was a lie.
Secondly, there is a well-known phenomenon in psychology known as the Dunning-Kruger effect, which states that the less competence or knowledge individuals have in an area, the more they will overestimate their competency and knowledge (e.g., as the DMSO series I’ve written has attracted more attention, an increasing number of DMSO hit pieces have been written and I’ve found that the more nonsensical, erroneous or misinformed the arguments presented are, the more confidently and aggressively their proponents espouse them and the more resistant they are to considering any conflicting data).
In medicine, there is a massive amount of information that needs to be learned, so in most cases doctors are forced to take short cuts throughout their training where again and again they assume if A is true then B is true without understanding exactly why A leads to B or how tentative the link can be and in which situations it does not apply. Likewise, when the public (especially members of the media) appraises medical information, rather than try to understand how A becomes B, they typically take the pronouncement of an expert (e.g., a doctor) that “A always leads to B” as all there is to say on the subject.
Since A often does not actually lead to B, and people do not like admitting they are wrong (especially if, like doctors, an incredible personal investment was required to attain the social status they hold), when confronted with inconsistencies in their beliefs, the typical response will be to double-down on their position rather than try to critically understand the additional data.
All of this, in short, encapsulates what I routinely observe when I see doctors or those aligned with “the science” defend (essentially-indefensible) aspects of vaccination.
Note: another common psychological mechanism at work, cognitive dissonance (not wanting to admit something you’ve invested yourself in was wrong), is particularly applicable to doctors, as it is a heavy burden to acknowledge you had harmed a significant number of people you willfully vaccinated.
Third, a strong argument can be made that societies cannot function without some type of unifying faith or spirituality (particularly since in the absence of one, people will frequently seek out one to adopt). In our culture, a rather peculiar situation emerged where religion was cast out by broad swaths of the society and replaced with science (under the belief it would create a fairer and more rational society) but the underlying need for a widespread faith was never addressed.
Because of this, much of science gradually morphed into the society’s religion, resulting in it claiming to be an objective arbiter of truth, but in reality, frequently being highly dogmatic and irrational as it seeks to establish its own monopoly over the truth (which has led to many labeling the current societal institution of science as “scientism”). As such, when science is discussed, religious terminology is often used by its proponents (e.g., “I believe in science,” “I believe in vaccines,” “anyone who denies climate change is reprehensible and must be silenced”).
The Religion of Medicine
Over the years, many have made the observation, medicine, by claiming dominion over life and death (and creating modern miracles like reviving the dead with cardiac resuscitation or awing the public with their ability to see through flesh with x-rays) has come to function as the foundation of the new religion of science.
Modern Medicine can’t survive without our faith, because Modern Medicine is neither an art nor a science. It’s a religion… The Church of Modern Medicine deals with the most puzzling phenomena: birth, death, and all the tricks our bodies play on us—Robert S. Mendelsohn
One of the first people who alerted me to this idea was Dr. Mendelsohn, who in his 1979 book, Confessions of a Medical Heretic argued that medicine was a dogmatic institution that prioritized authority, control, and ritualistic practices (which were treated as infallible doctrines requiring blind obedience from patients) over patient well-being, data transparency, and evidence-based care. There, he:
•Highlighted “unwritten rules” in medicine, such as doctors compulsively rushing to prescribe new drugs before their side effects are fully known, as examples of this rigid, faith-like adherence to protocol over science (particularly since debacles routinely followed this blind faith in new pharmaceutical drugs).
•Demonstrated how many routine practices and procedures caused significantly more harm than benefit (e.g., x-rays for tonsillitis later creating thyroid cancer) but could not be challenged due to the dogmatic nature of medicine, leading to similar debacles being repeated in each ensuing decade.
•Demonstrated that many illnesses that are routinely treated with (harmful) interventions would recover on their own, especially if augmented with simple natural healing practices.
•Argued that medicine’s tendency to withhold foundational medical information from the public (hence forcing them to trust the doctor’s opinion rather than their own judgement) was fundamentally unethical.
Note: this critique was raised in the pre-internet age where medical journal information was not widely available to the public. I believe this in part explains why journal articles published at this time (many of which I cite in this newsletter) were much more candid, whereas in later decades information which potentially incriminated the medical profession rarely made it to publication.
•Argued medicine’s compulsion to “do something” as a faith-based impulse rather than rational care, equating medical overreach with religious zeal that harms believers.
•Noted that in addition to patients being attacked for challenging the faith, doctors who did were treated as heretics and cast out (e.g., by being forced to resign from the hospitals they worked at).
Nowhere does the Church’s Inquisition emerge as clearly as it does through the drugging of children as a means of control… Modern Medicine sets up its Inquisition to define behavior which doesn’t conform as sick.
Mendelsohn’s work, in turn, was hugely impactful and played a huge role in shifting medicine away from the paternalistic model to one where patients began to be provided with data and allowed to play a role in deciding what care was optimal for them. For example, he made numerous highly impactful appearances on national television appearances such as this 1983 debate on the dangers of vaccines.
Note: over the last month, I compiled 54 other news segments that were aired on the dangers of vaccines that would never be aired now (and can be viewed here).
Nonetheless, many of the issues Mendelsohn highlighted persist to the present day. For example, doctors who tried to prevent COVID patients from dying by deviating from the ineffective remdesivir protocols were kicked out of their hospitals, the experimental mRNA vaccines were embraced with an unstoppable religious zeal by the medical community despite very little being known about them at the time and data on the safety or efficacy of the COVID vaccines was withheld from the public despite continual efforts and lawsuits to obtain them.
In his book, he also highlighted specific techniques utilized by medicine such as:
•Doctors had taken the place of priests in the church and that many deliberate parallels existed between the two (e.g., at medical visits you were expected to confidentially confess your sins to them and the white coats doctors wore as emissaries of science were modern robes of a priest while stethoscopes serve as their religious badges). Because of this, “the doctor-priest gets away with a lot because he can claim to be up against the very forces of evil.”
•Research being the endless ritualistic toil people used to pledge allegiance to the faith (“Research is OK as long as you don’t act on it”).
•Hospitals functioned as the temples of the church of medicine.
•Medical insurance was functionally similar to the indulgences members paid to support a religion.
•Drugs, regardless of their harms, were treated like communion wafers and unnecessary surgeries were effectively ritualistic mutilation—both of which created loyalty to the church of modern medicine.
•Infant formula was a “blessed” food in order to justify severing mothers from (much healthier) breast feeding.
•Vaccines were the holy water used to baptize you into the faith.
Witness the vigor with which the State proselytizes Modern Medicine’s line of Holy Waters… Everybody needs—and gets—the Holy Waters: routine silver nitrate in the eyes of the newborn, routine intravenous fluids to laboring mothers and other hospital patients, routine immunizations, and fluoridation of water supplies… That same fierce compulsion motivates the priests of Modern Medicine in slapping their Holy Waters on their patients.
You have to submit to the Church in order to go to school. They won’t let you in the door unless you can prove that you’ve received all the sacramental immunizations.
Here, vaccines symbolize initiation and ongoing devotion, with refusal risking exclusion or accusations of neglect.
Of these points, I spent by far the most time pondering his argument vaccines were medicine’s holy water, as:
•Every medical student (and now healthcare workers too) are required to be fully vaccinated—both filtering out those not aligned with medicine’s dogmas and making those who submit to them be much more inclined to push them on patients.
•Vaccines greatly increase the likelihood of chronic illnesses (typically a 3-10X increase), causing recipients to become lifelong adherents to medicine and the drugs it provides to manage those symptoms.
•Vaccines are one of the initial traumatic experiences infants experience, and to some extent repattern the nervous into a shocked and disconnected state where it’s harder to have a fulfilling engagement with life and those around you (hence making them more likely to seek salvation in the materialistic paradigm offered by science).
For a long time, the religious nature of the vaccination has been a relatively unknown and taboo topic to discuss, but fortunately, in recent days that has shifted. Here for example, Tucker Carlson and Cheryl Hines gave millions of viewers one of the most poignant explanations I’ve seen for why vaccination is ultimately a religious ritual:
Note: the Diego mural deifying vaccination Tucker was referring to is this Detroit one which was created in 1932-1933.
 |
Vaccines Amen
Recently Aaron Siri published, Vaccines Amen, an excellent book, which to my knowledge, makes the best comparison between medicine and religion since Mendelsohn’s 1979 work (but instead restricts its focus to the religion around vaccines as the dogma in the other areas has somewhat declined since Mendelsohn’s time).
This book, briefly attempted to highlight the religious nature of vaccines by showing how over and over:
•The words of a small number of trusted authorities are taken as a dogmatic truth everyone else in the medical field copies—despite most of their statements not being supported by evidence or logic. Siri, remarkably, was able to depose the godfather of America’s current vaccine program (who shaped most of the current vaccine spokespersons across the country like Paul Offit), and during that deposition, showed the critical gaps in his duplicitous reasoning which came to define the practice of vaccination.
Note: Siri also made the point that most of the high priests of vaccination (who all parrot the same talking points) only got to where they were due to pharmaceutical funding which is selectively allocated to those who reinforce the orthodoxy). Likewise, he highlighted how individuals like Offit are treated with a blind trust by the medical profession, media, and government regulators, allowing the illogical beliefs they promulgate, like all good propaganda, be completely shielded from scrutiny.
•How illogical and blatantly inconsistent positions are taken to argue that vaccines are safe and effective so that nearly identical types of evidence are accepted if they support that belief but rejected if they refute it—hence making the evidence underlying this belief system subjective to the point of being worthless. Siri, in turn highlights the glaring contradictions (or extremely consequential positions being repeatedly taken in the absence of any supporting evidence) with the phrase “Vaccines, Amen”—which does aptly sum up the situation.
Note: “Vaccines Amen” is also used to highlight other facets of vaccine zealotry such as censoring those who question vaccines or forcing people to vaccinate rather than winning them over with logical arguments.
•How vaccine safety research is layered with endless assumptions vaccines must be completely safe (which conceals all the harms they actually cause) but that research (which never actually proved safety) is presented as ironclad proof vaccines are both safe and effective.
The Absence of Evidence is Not the Evidence of Absence
Due to the high toxicity of vaccines, it is nearly impossible to design studies which do not show vaccines sicken their recipients. Because of this, the medical community’s strategy has been to block studies comparing vaccinated to unvaccinated from ever being produced.
For example, whenever people attempt to conduct placebo controlled trials of vaccines, they are vehemently rejected by the medical field as being unethical to perform because it denies children in the (tiny) placebo group, a “life saving” vaccine—despite it being far more unethical to inject every child in the country with a vaccine of unknown safety or efficacy (where real concerns of safety exist).
Conversely, whenever an (“ethical”) study is conducted (e.g., retrospectively comparing the health of vaccinated to unvaccinated within large datasets) and shows vaccine injures are real, the study is rejected for being “non-controlled” with the argument being a controlled trial needs to be done to assess this—despite those trials being banned for “ethical” reasons. Further highlighting this absurdity:
•When (uncontrolled) databases show something demonstrating vaccine safety, this is always treated as proof vaccines are safe.
•Large datasets exist which can (ethically) compare the vaccinated to unvaccinated. In all cases, the public is never given access to the datasets despite individuals like Siri going to great lengths to obtain them (with the common argument being that it’s unethical to share personal health information, despite this never being an issue for pro-vaccine researchers who assess large databases).
•When individuals independently conduct studies comparing vaccinated to unvaccinated children and demonstrate harm, those studies get retracted and the investigators are often targeted by medical boards (e.g., Paul Thomas lost his Oregon medical license for this).
•It would be very easy to prove vaccines were “safe and effective” by conducting a study comparing the vaccinated to unvaccinated—yet despite decades of pleas and an ever increasing loss of trust in vaccines they are never done—or if done, never published.
Note: recently, we learned one of the strongest proofs of this, as a physician who wielded immense prestige and had a track record of challenging entrenched interests agreed to conduct a vaccinated vs. unvaccinated study to prove vaccines were safe and then publish the results regardless of what they showed (as he was certain they would show vaccines were safe). Once its data irrefutably showed vaccines were immensely dangerous, he refused to publish the study and apologetically admitted to a hidden camera he did that to protect himself.
Since propaganda relies upon “logical sounding” arguments rather than logical ones, this status quo has hence remained the societal standards for generations and been shielded from all arguments against it. As such, two critically important points of logic rarely enter the discussion.
First, it is assumed that because no evidence of vaccine injury has emerged despite them “being the most studied medical product in existence” that means they are completely safe—when in reality, that absence of (widely-accepted) evidence is entirely a product of a refusal to look for it. This in turn harkens back to the famous phrase “the absence of evidence is not the evidence of absence” (something I continually hear in my mind whenever vaccine zealots default to this argument).
Second, I’ve long observed many problems in science originate from an erroneous interpretation of a philosophical concept. For example, the modern FDA arose from a 1962 law which stipulated drugs should be approved on the basis of a “well-controlled” investigation, after which “well-controlled” (which was never defined) was habitually interpreted to mean costly trials only industry could afford to conduct. As a result, (accurate) trials independent parties could conduct are routinely dismissed by regulators and the medical community, while large “blinded” trials that are highly inaccurate and biased (due to the industry funding they require) are essentially completely shielded from scrutiny (e.g., numerous trial participants and clinical investigators testified that both the HPV and COVID-19 trials were doctored but the FDA never did anything).
Note: RCT fundamentalism (the refusal to consider anything besides randomized controlled trials) is highly misguided as smaller observational unblinded trials will typically yield the same results as large (non-corrupt) RCTs (proven by this 2014 Cochrane Review), especially if the effect of a drug is significant (rather than a tiny one that can only be detected in a large controlled study and hence is likely inconsequential). As a parallel to this Cochrane review, I have consistently found the most successful people in life are those able to detect signals in preliminary data and then act upon them rather than waiting for the crowd to sanction the choice (e.g., the best doctors I knew recognized the COVID vaccines were incredibly dangerous within a month of them being on the market—whereas many physicians I know still will not acknowledge this).
Recognizing that medicine had become a dogmatic ideology incapable of overturning harmful practices, medical dissidents attempted to transform medicine by instilling the framework medical practice should be dictated by scientific evidence rather than expert opinion, something which was greatly needed and allowed numerous dysfunctional medical practices to at last be discarded.
Unfortunately, the pharmaceutical industry rapidly realized this meant immense profits could be made if they invested in monopolizing the evidence by:
•Buying out the medical journals, thereby making it impossible for anything which threatened their interests to be published (and become evidence), while simultaneously allowing anything which supported industry interests to be published regardless of how poorly put together it was (e.g., numerous papers using completely nonsensical datasets were published in the top medical journals and used to stop global trials of off-patent COVID treatments—then eventually were retracted once enough of us pointed out their datasets were clearly fabricated).
•Instilling the belief we should trust someone else’s curated summary of the data rather than being able to examine the data ourselves (e.g., during COVID, they kept telling us the data showed the vaccines were safe and effective, but refused to ever give it to us, and in the instances where we eventually did through court orders or luck, we saw that they lied about what was actually in the raw data).
•Using the mass media to enshrining the societal belief the pronouncement from “expert” about the evidence was equivalent to the evidence itself.
As such, mirroring the general trend of science in our culture, evidence-based medicine’s framework transitioned into a belief, and has gradually reverted to the dogmatic system which preceded it. For this reason, I believe there is significant merit at examining its original (1996) definition:
Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. By individual clinical expertise we mean the proficiency and judgment that individual clinicians acquire through clinical experience and clinical practice.
Increased expertise is reflected in many ways, but especially in more effective and efficient diagnosis and in the more thoughtful identification and compassionate use of individual patients’ predicaments, rights, and preferences in making clinical decisions about their care. By best available external clinical evidence we mean clinically relevant research, often from the basic sciences of medicine, but especially from patient centered clinical research into the accuracy and precision of diagnostic tests (including the clinical examination), the power of prognostic markers, and the efficacy and safety of therapeutic, rehabilitative, and preventive regimens. External clinical evidence both invalidates previously accepted diagnostic tests and treatments and replaces them with new ones that are more powerful, more accurate, more efficacious, and safer.
In my eyes, there are two major misinterpretations of this. First, as many have pointed out, mandating a therapy (e.g., vaccines) is irreconcilable with respecting “individual patients’ predicaments, rights, and preferences.”
Secondly, “best available evidence” was redefined to mean “highly credible” data obtained by large (costly) randomized controlled trials and endorsed by experts, rather than the best available data currently existing on a topic. As such, I believe the argument “you cannot accept all the observational studies showing vaccines cause harm because they aren’t robust placebo-controlled trials” is a gross distortion of the (explicit) intent behind evidence based medicine.
Rather, the correct interpretation is that currently, the observational studies comparing vaccinated to unvaccinated children constitute the best available evidence (since nothing “better” has been done), and their conclusion must be the standard for determining medical practice until “better” (e.g., placebo controlled) trials are done and they refute the observational studies. As we can see with the subject of vaccine safety, this is hugely consequential as this redefining has allowed vaccine promoters to both stonewall foundational research into vaccines while simultaneously claiming all which already exists “doesn’t count.”
Or to quote Vaccines Amen:
It is not surprising that pharmaceutical products, including vaccines, can cause harm. What is deeply concerning is that vaccine proponents often assert a vaccine does not cause a claimed harm without evidence to support their claim. Even when millions report a specific harm associated with a vaccine, Dr. Plotkin and his followers maintain that vaccines do not cause that harm, despite lacking evidence to substantiate their position.
Returning to the earlier example, when I asked Dr. Plotkin whether the hepatitis B vaccine can cause encephalitis, he replied, “No, I would say definitely not.” However, when confronted with the Institute of Medicine (IOM) report, which provided no support for his conclusion, he did not retract his statement. Instead, he doubled down on this unscientific stance. When pressed further, he acknowledged that proving a negative requires more data than proving a positive, but this does not justify claiming a vaccine does not cause a commonly reported harm without evidence. He maintained this position even after admitting that a properly designed clinical trial could determine whether a vaccine causes a specific harm.
Likewise, when Siri tried to obtain the data proving vaccines were safe:
After years of asking, requesting, demanding, deposing, and suing key entities and figures in the vaccine industry and federal health agencies, no one remains to approach for the supposed “mountain of studies” claiming that infant vaccines do not cause autism. The assertion of such a vast body of evidence is unbelievable, yet health officials who claim this mountain exists cannot identify a single study to support the claim that infant vaccines do not cause autism. Not one study exists. What is clear, requiring no leap of faith, is that the claim vaccines do not cause autism is not based on science but on ideological belief.
This reminds me of what former House Representative Dr. Dave Weldon wrote in 2007: “When I first tasked my staff with investigating federal vaccine safety research, we received confused responses and blank stares from federal officials. The FDA directed us to the CDC, stating that the CDC conducted most vaccine safety research. The CDC referred us to the NIH, which then referred us back to the CDC.
Incredibly, the only study identified by the CDC that examined a vaccine given during the first year of life was one that found an association between the DTaP vaccine and autism.
Note: the Institute of Medicine (IOM) is a private organization which is often treated as the gold standard for assessing scientific controversies (even though they typically whitewash the subject at hand) and has written numerous widely cited reports on the safety of vaccines (with their 1994 report and the 2012 report being two of the most well known). These reports stated that there was insufficient evidence to definitively support a link between vaccines and serious injury and that it was concerning this research had not been done. However, as this absence of evidence was widely interpreted as evidence of absence (even with the IOM noting one study showed a link between vaccines and autism), the IOM reports have been brandished as proof vaccines are safe despite that being very far from what the IOM actually stated.
Burying Evidence
One of the key points Siri’s book are the elaborate lengths the vaccine industry goes through to doctor the data on vaccine safety.
For example, in clinical trials for vaccines, they are always conducted for very short periods (e.g., the studies for the hepatitis B vaccines we give every newborn only monitored for side effects for 4-5 days), making it impossible to detect long term side effects, and in almost all studies, rather than the vaccine being tested against saline placebos, vaccines are tested against injurious substances which are assumed to be safe, after which safety is assessed by comparing the injury rates between two groups. To illustrate what a massive scam this is, consider the following scenarios:
Fake “Placebos”
A new vaccine is sometimes tested against an “inert” placebo which contains the vaccine’s harmful adjuvant. If the vaccine has a 10% rate of serious injuries, and the “placebo” has a 9% rate of serious injuries, the 1% difference is within the margin of error and hence assumed to be due to chance rather than the vaccine.
For example, here is some of the data from the HPV vaccine trial (which used a harmful aluminum adjuvant as the placebo:
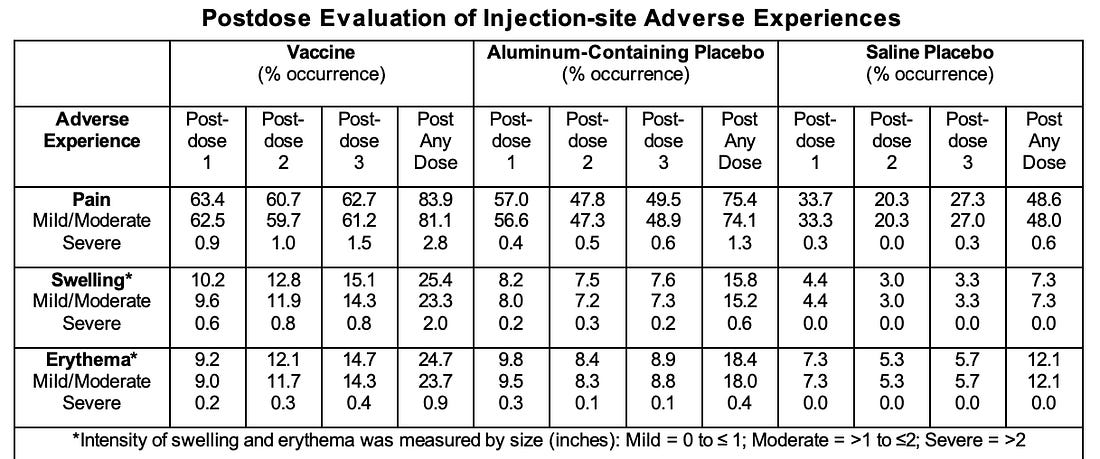 |
Similarly, in the initial Gardasil trials, out of 21,458 10 vaccine recipients and 7 “placebo” recipients died including 7 from car accidents (which can be triggered by POTS causing drivers to pass out). However, despite the Gardasil death rate (8.5 per 10,000) and the “placebo” death rate (7.2 per 10,000) being almost twice the background death rate in girls and young women (4.37 per 10,000), the FDA was not concerned.
Note: as these trials selectively recruit for healthy participants, the expected death rate should have been even lower than 4.37 per 10,000 in a true placebo group).
Vaccine “Placebos”
Prior to licensure, the control group in the main study for Prevnar 7 received another experimental vaccine instead of a placebo. Both vaccines provoked similar adverse effects, reducing the ability to detect differences in safety outcomes between the two groups.
It is routine for the “placebo” given for a vaccine during a vaccine trial to be another vaccine rather than an actual placebo, creating a scenario where the tested vaccine can only be proven harmful if it is more harmful than a “safe vaccine” which already has a high injury rate. If you take a step back, this is particularly absurd as the previously existing argument “it’s unethical to deny children a lifesaving vaccine” (which would be necessary to conduct a placebo controlled trial) goes out the window here as the substitute vaccine cannot prevent the target disease you need to prevent (since it’s for some another disease).
Note: in many cases, vaccines make one more likely to catch illnesses, as they create a temporary immune suppression which makes you less able to resist infections besides those the vaccines are hyper-priming your immune system to focus on (hence why people frequently get the flu after flu shots). I have long wondered if this is part of the rationale for using vaccines as placebos since it also artificially inflates the efficacy of the tested vaccine as the comparison group becomes an immune-suppressed population with higher rates of the infectious illness.
Likewise, in many cases, these vaccine placebos are chained together to normalize and conceal a high rate of injury and death. Leading to situations similar to this:
- First study: Vaccine A (8% injury rate), no comparison—but Vaccine A is just assumed “safe.”
- Second study: Vaccine B (10%) vs. “safe” Vaccine A (8%) — Vaccine B is assumed to have a 2% injury rate and hence is “safe.”
- Third study: Vaccine C (11.5%) vs. “safe” Vaccine B (10%) —Vaccine C is assumed to have a 1.5% injury rate and hence is “safe.”
- Fourth study: Vaccine D (14%) vs. “safe” Vaccine C (11.5%) — Vaccine D is assumed to have a 2.5% injury rate (14-11.5) and again is “safe.”
If you consider either situation, it’s obvious this situation is absurd as a 1-3% injury rate would likely be being seen were an actual placebo being used, and anything above that (e.g., 14%) would be harm clearly attributable to the vaccine. However—that is the actual status quo we’ve had for decades (and why the medical community had such a hysterical reaction to RFK Jr. deciding future vaccines would need to be tested against placebo for approval).
Note: Del Bigtree gives an excellent example of this being done in the above video. Likewise, due to frequently having to challenge the claim “vaccines are complete safe” in court, Aaron Siri’s team has gone through the licensure studies and successfully mapped out how this “placebo” pyramid scheme underlies the safety for many widely used vaccines and that we have no actual data to establish the safety of many of the products we inject into our children.
Sadly, doctoring clinical trials is well-honed art, and as a result, the same fraudulent tactics are repeatedly utilized throughout the pharmaceutical industry. As such, in addition to having a narrow window to monitor for side effects (thereby hiding the chronic illnesses vaccines cause) and having vaccines be compared to a baseline where a large amount of sickness and injury is “nothing to be concerned about” we also repeatedly see:
•”Placebo groups” somehow becoming unblinded to the investigators, resulting in the efficacy being exaggerated in the test group, and harms downplayed in the control group. The best example of this I’ve seen was in the COVID trials, as data in the trials indicated they had been unblinded, and whistleblowers came forward stating probable COVID cases weren’t tested for in the vaccine group (whereas placebo recipients consistently were tested with COVID tests that frequently had false positives) while adverse reactions in vaccine recipients frequently were not recorded.
Note: a good case can be made a significant amount of the COVID vaccine’s benefit was an artifact of biased trial design.
•It being almost impossible to report adverse reactions occurring that are not “expected reactions” being monitored for (ie. fever or fatigue)—something we also saw through the COVID vaccine trials and within the CDC’s system that was created to monitor the vaccines for safety.
•Pharmaceutical companies being permitted to reclassify injuries that occur to make them seem less bad (e.g., COVID trial participants testified that a severe cancer was reclassified as enlarged lymph nodes and a permanent disability was reclassified as “functional abdominal pain”).
Note: in many cases, they also obfuscate adverse events to point it’s impossible to determine the extent of the harm (e.g., in Gardasil’s trial data, Merck disclosed that 49.6% of vaccine participants developed a “New Medical Condition,” 2.3% of which were categorized as “potentially indicative of a systemic autoimmune disorder”).
•Investigators having the discretion to determine if a reaction was related to the test product, and if they feel it is unrelated, it is accepted as not being related (e.g., there are many shocking documented examples of this within the Gardasil and COVID trials of crippling and highly unusual illnesses immediately following vaccination being deemed “unrelated”).
Sadly, as mentioned before, these issues are not unique to vaccines. For example, recently Secretary Kennedy shared a post highlighting the decades of suppressed evidence SSRIs can cause violent behavior:
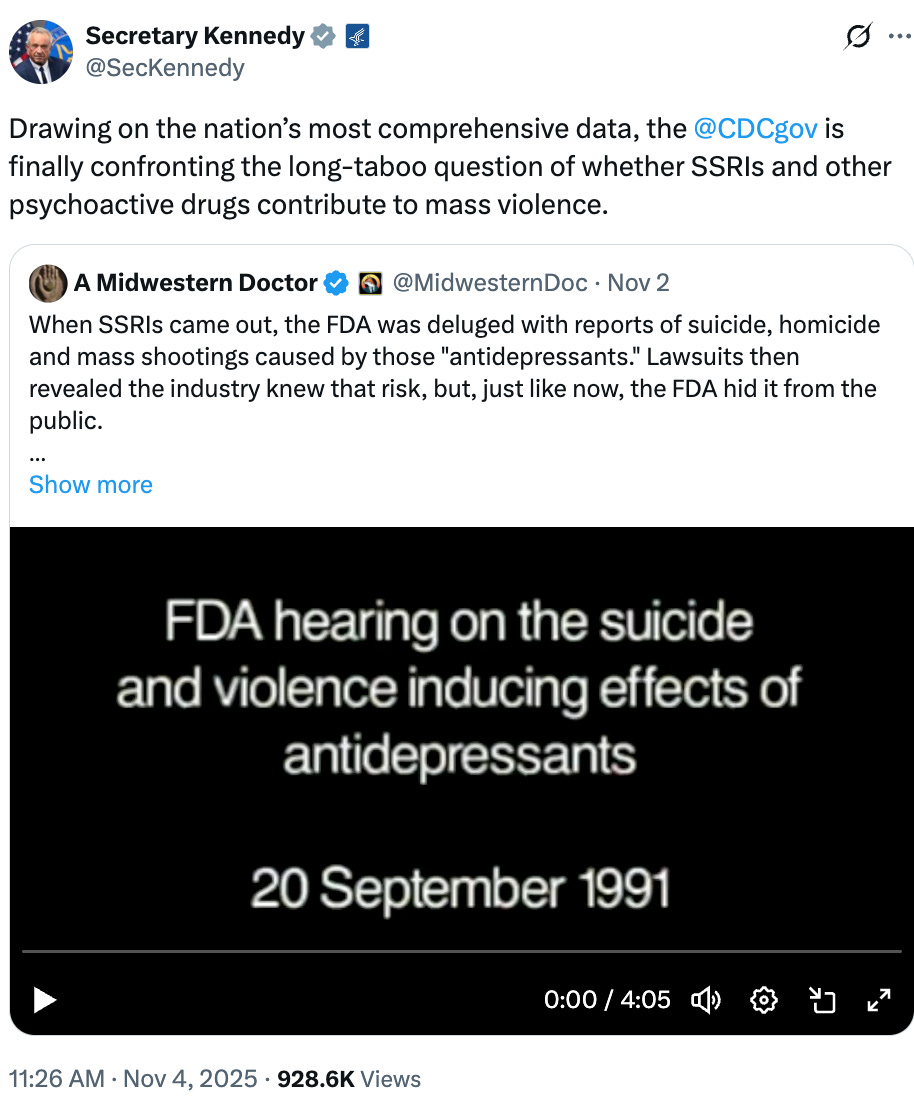 |
One comment on the thread (from a fairly open-minded doctor) caught my eye, as it effectively said: yes violent SSRI behavior does occur during clinical trials, but despite trials being the place where we are supposed to assess if a correlation indeed occurs, we still will not deem the events to be linked to SSRIs.
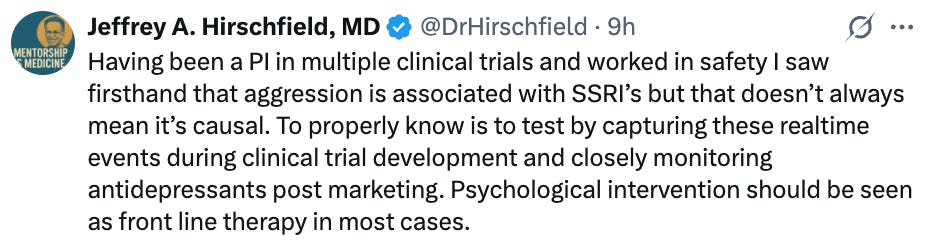 |
Note: PI’s (principal investigators) are the ones with the authority to determine if injuries are linked to the tested drug product.
Regulatory Capture
A variety of safeguards (e.g., scrutiny from the scientific field or consumers choosing to boycott a bad product) are supposed to exist to prevent something harmful from being forced upon the entire public. Yet, as we’ve come to see, the faith and systematic lobbying behind the vaccine industry has allowed every safeguard to be bypassed and replaced with the belief “vaccines are safe and effective” and laws that enshrine the industry’s monopoly (e.g., vaccine mandates).
A key point Siri made was that since the 1986 National Childhood Vaccine Injury Act took away the standard oversight an industry faces (the threat of liability lawsuits incentivizing developing safer products), the Department of Health and Human Services assumed that role, and as such, a variety of provisions were put into the act which allowed it to conduct the oversight which would ensure safer vaccines were brought to market. However:
On May 24, 2014, Dr. Thompson stated that the CDC is paralyzed by anything related to autism because they fear discovering associations. This fear may stem from the fact that HHS has conceded, or been required by the vaccine court, to pay financial compensation in at least a dozen cases where children developed brain, neurological, or immune dysfunction diagnosed as autism after receiving vaccines on HHS’s childhood schedule. Some of these damage awards reached millions of dollars. If a single HHS study found that one in five autism cases was linked to vaccines, it could result in approximately $1.3 trillion in liability. For context, the entire federal budget in 2017 was $3.3 trillion. The potential damage to HHS’s reputation if certain vaccines were found to cause a significant portion of autism cases provides a strong incentive for HHS to avoid funding basic scientific research to determine whether its childhood vaccine schedule contributes to autism.
Unfortunately, almost all of those 1986 Act’s provisions were ultimately at the discretion of the Secretary of Health and Human Services. Not surprisingly, again and again, those required provisions were not implemented (which in many cases Siri was able to prove through lawsuits) and very little has been done to develop safer vaccines (best illustrated by an incredibly dangerous and experimental mRNA vaccine being mandated upon the entire population despite the existing scientific evidence arguing strongly against doing so).
For example, in Vaccines Amen, Aaron Siri shows that that:
•FOIA’d emails showed that the head of the CDC’s Immunization Safety Office routinely communicated with the pharmaceutical industry to help set national vaccine policy (while simultaneously stonewalling citizen groups advocating for vaccine safety).
•The (authoritative) reports the CDC publishes are heavily scrutinized within the agency to ensure they only release data which supports the notion vaccines are safe, effective, and necessary.
•Many members of the CDC and the independent advisory panels which assess vaccines view the authorities within the vaccination industry (particularly Stanley Plotkin) with such reverence that their claims are rarely subject to basic scrutiny regardless of how absurd they are.
•Since lackluster standards exist to ensure vaccines brought to market are safe (e.g., there are no placebo trials due to the “ethical” issues involved in conducting them), the proposed solution to address this is post-marketing surveillance (e.g., robust monitoring systems being able to flag dangerous vaccines so they can be taken off the market). Unfortunately, since all of that is at the CDC and FDA’s discretion, and they “know” vaccines are safe, this virtually never happens as every signal of harm is dismissed (best demonstrated by what we witnessed throughout COVID-19).
•When irrefutable examples of vaccine injury arise, the typical priority is to find ways to cover up the bad publicity rather than address the issues (e.g., Siri cited UNICEF working with the CDC to cover up the backlash from data showing their vaccine program was killing children rather than change the vaccination program itself). Similarly:
Scotland’s COVID-19 data revealed that vaccinated individuals had twice as many cases as the unvaccinated. Instead of addressing the vaccines’ potential shortcomings, Scottish health authorities stopped issuing these reports. They were willing to publish data when it showed higher infection rates among the unvaccinated, but when the data indicated that the vaccinated were more likely to be infected, contradicting their narrative, they ceased publication.
Shattering Illusions
When you attempt to dissect the vaccine mythology (particularly when challenging them in court), you will frequently run into so many contradictory logical positions it is often impossible to make sense of a coherent logic behind them. Siri, however, makes a good case the unifying thread behind all of it is an “a priori” assumption vaccines that are always safe (which then serves as the foundational premise all other arguments and data on vaccination are derived from).
One of the best proofs I’ve seen from this recently came from Gavin DeBecker’s excellent book Forbidden Facts which demonstrates through leaked records that the IOM report on vaccine safety showed that the members of the “independent panel” of experts were told at the start that they needed to not provide evidence vaccines were harmful. As such, the committee repeatedly went out of their ways to concoct ways to dismiss the existing evidence of harm without directly lying (hence why things like the “absence of evidence” gambit were so popular as it allowed them to imply vaccine safety without directly stating a falsehood) and in those transcripts openly acknowledged the dishonesty of what they were doing.
Because vaccines have such a high rate of injury (and conversely their benefit is so small), I have long felt the only way the existing paradigm can be sustained is by having the majority of the population believe vaccines are “safe and effective” and prohibiting any debate on the subject, as the moment that debate emerges, the nonsensical contradictions used to justify the existing paradigm become immediately apparent.
Note: as a parallel, early in this publication, I attempted to draw attention to the robust evidence linking SSRI antidepressants to mass shootings as I felt clearly making the case for that had a good chance of going viral (which it ultimately did due to Tucker Carlson’s team somehow seeing it and him then discussing the topic on Fox News), after which that article was ultimately seen by over a million people and the idea became promoted by many large conservative influencers. Once this happened, the issue became politicized, at which point people became interested in justifying their positions, and the clear dangers of SSRIs (which are far more common than the SSRI trigged murders) at last became an open topic of debate and the entire cultural perception towards SSRIs has rapidly shifted to a degree I previously never thought could ever happen.
Consider for a moment the absurdity of the current paradigm where our society has been led to accept that vaccines are “so safe” you:
•Cannot sue the manufacturer if you are injured by a defective product.
•Can be mandated to take them if you do not feel they are “safe and effective” enough to voluntarily take them.
•Cannot see the data proving they are safe and effective.
•Cannot request for “unethical” placebo trials to be conducted to determine if they are safe and effective.
Yet, despite all the games these people have played around vaccines to enshrine this state of affairs, there is one unshakeable fact they still can’t overcome—once someone (or an immediately family member) is severely injured by a vaccine, no amount of propaganda can sweep away their lived reality of a vaccine injury, particularly if numerous people they speak to have the identical experience (e.g., in a recent interview with Mary Talley Bowdenseen by millions of people, Tucker Carlson noted his son got Guillain-Barré syndrome from an [unnecessary] flu shot).
To sell the experimental spike protein-producing gene therapies, a decision was made to market these injections as “vaccines” and use the trust in the vaccine brand to overcome the rational skepticism the public would otherwise have to a product of this nature. This “worked” (hence why 81% of the population got at least one COVID vaccine and the COVID injections became one of the most profitable products in history).
However, this greed backfired as the high rate of injury from them broke the unshakable trust in the vaccine brand the industry has relied upon for decades. Because of this, people (including lawmakers) are at last calling out the absurdities that have been used to sell everyone vaccines.
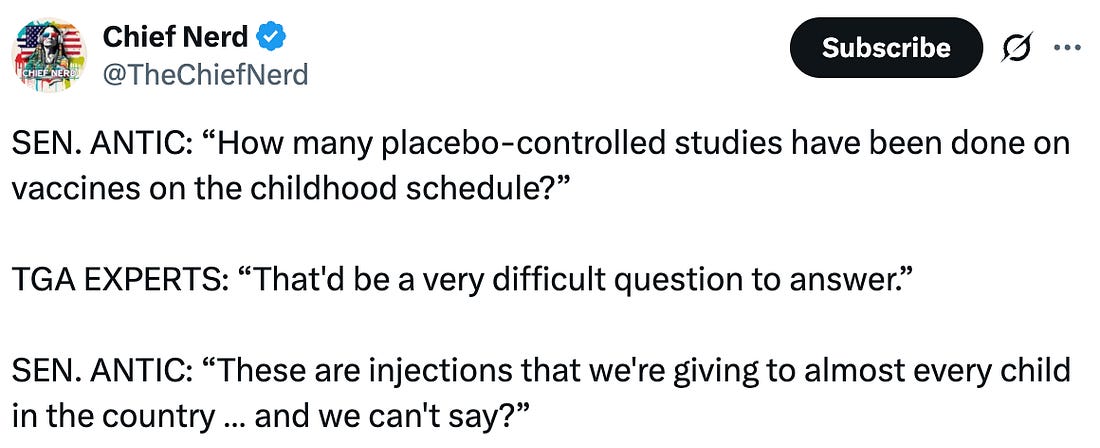 |
There has never been an opportunity like this in our lifetimes and for that reason, I believe it is critical to do what we can to get this message out and support people who are doing excellent work to shift this issue (e.g., I wrote this article in part because of the vital work Aaron Siri has done over the years to support vaccine safety and in part because his book ties together critical pieces around the religious ritual of vaccination alongside critical covering aspects of the vaccine issue I never came across despite my own extensive research).
Conclusion
Ultimately, there are always two ways you can sell a product to someone. The more commonly used option is by telling them to buy it, then using the social pressure and propaganda to pressure them into going along with the crowd, while the other is to provide them with the data that will allow them to rationally decide it makes sense to adopt your position.
I have always advocated for the latter (which is why this newsletter aims to appeal to self-directed readers with clearly presented information rather than emotionally pressuring people to adopt my beliefs) and have long sought out the self-directed members of the population who made an effort to see things for what they were rather than what they’d been told to see.
However, due to how overused the propaganda to sell the injurious vaccines was, a shift was catalyzed in our culture to begin prioritizing a self-directed determination of truth that remarkably occurred at the same time uncensored platforms became available for the alternative media. This hence allowed something I never imagined to emerge; public interest in the alternative media allowing it to rapidly displace the mass media and begin widely covering previously forbidden topics like the harms of vaccination.
That shift has been directly catalyzed by each of you, and I thank you deeply both for the support you’ve given independent authors like me, and for the wide range of previously taboo topics that support is allowing to at last emerge into the public consciousness.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.




Leave a Reply
You must be logged in to post a comment.