Bravery (and Humility) is Needed to do Proper Medical Science
May 4 | Posted by mrossol | Math/Statistics, Medicine, Transparency[non]| JOHN MANDROLA MAY 4, 2026 |
I am not an orthopedic surgeon. Maybe you aren’t one either. But as a sports enthusiast, I’ve had acute joint pain of one sort or another.
Maybe you’ve been told something is torn. A torn meniscus, for instance. I don’t know what a meniscus is, but it being torn does not sound good. It’s like “bone-on-bone.” Such phrasing leads the brain to the idea that fixing is required.
Sensible Medicine is reader supported and free of industry influence. Please consider becoming a free or paid subscriber.
Last week in the New England Journal of Medicine, the FInnish team of investigators known as the FIDELITY trial investigators reported 10-year results of their placebo-controlled randomized controlled trial of arthroscopic partial meniscectomy vs placebo surgery. The original results came in 2013.
A word on “placebo” surgery. This is sometimes referred as a sham surgery. But I think that’s too harsh a word. Because if the actual surgery cannot pass muster over a placebo surgery, then the actual surgery should be called a sham.
Here was the Consort diagram for FIDELITY
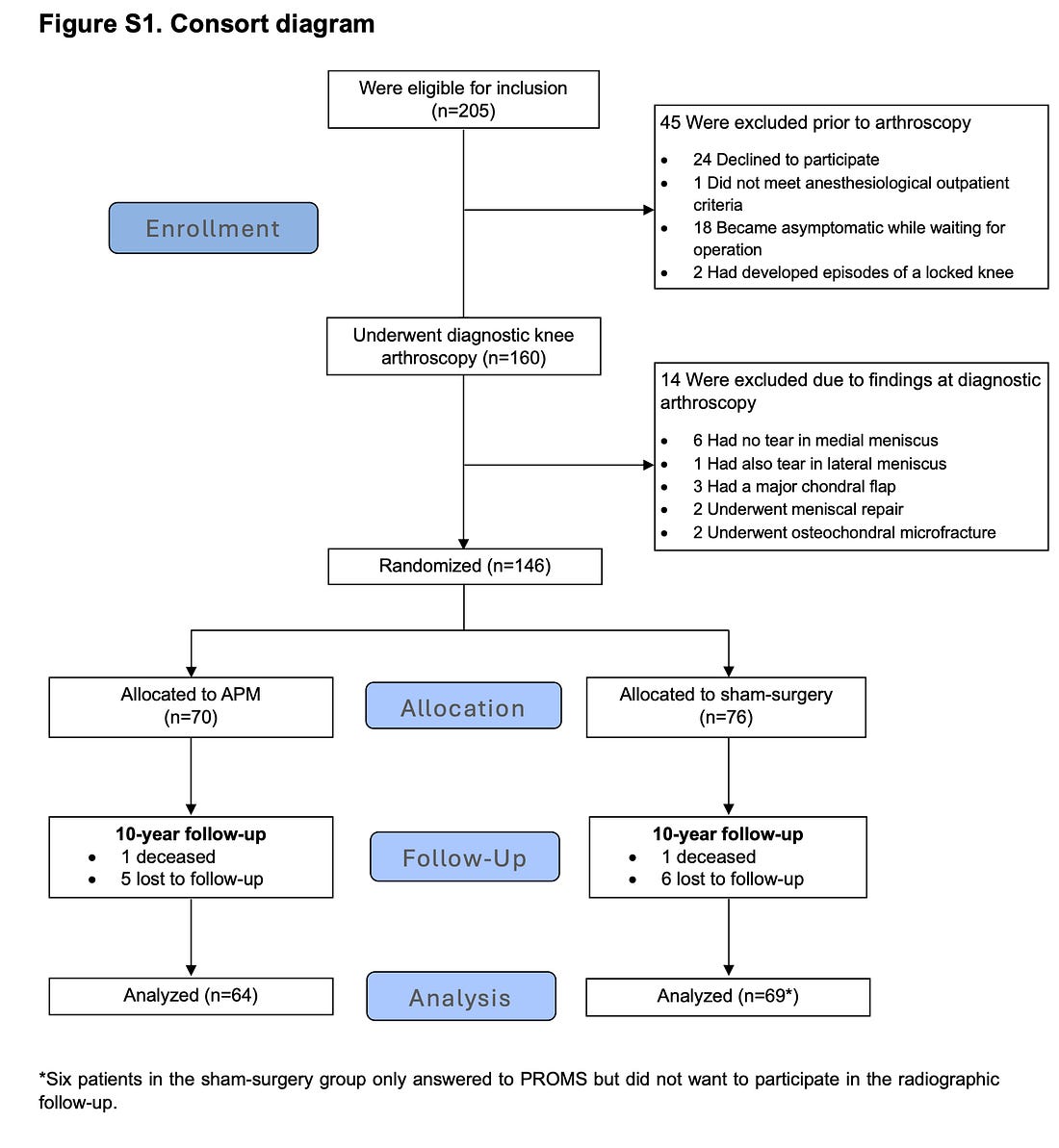
Notable in this trial was the young age (≈ 52) and exclusion if there was significant arthritis.
First was a diagnostic arthroscopy. Then randomization. Active arm surgery included removal of all loose, weak fragments as well as unstable meniscus with preservation of as much of the meniscus as possible.
For the sham surgery, a standard arthroscopic partial meniscectomy was simulated. To mimic the sensations and sounds of a true arthroscopic partial meniscectomy, the surgeon asked for all instruments, manipulated the knee as if an arthroscopic partial meniscectomy was being performed, pushed a mechanized shaver (without the blade) firmly against the patella (outside the knee), and used suction. The patient was also kept in the operating room for the amount of time required to perform an actual arthroscopic partial meniscectomy.
Outcomes were three pain scores. Their names aren’t critical. But all three were not statistically different. Critically, patients could not identify their treatment arm; blinding had worked.
In the 10-year radiological assessment. 81% of the patients in the operative arm had progressed to have arthritis vs 70% in the placebo arm. This barely missed statistical significance. More patients in the placebo arm reported satisfaction (84% vs 75%). More patients in the surgery arm progressed to high tibial osteotomy or total knee replacement (12% vs 4%).
Comments
The first thing that pops in my head is: what if these researchers (and patients) were not so bold. An ineffective procedure would have remained popular, with costs into the billions, and if the trends in this study are true, increasing numbers of people would progress to knee replacement. AKA: harm.
Having visited Northern Europe many times, I am struck by their research culture. You walk through a hospital in Copenhagen and multiple patients are enrolled in clinical trials. My Danish colleagues tell me that patients are open to being in studies.
We don’t see this as much here in the US. I get the sense that American patients would be less likely to enroll in a placebo surgery because they’d have the mindset that the doctor must know a surgery works lest she or he would not do it. Maybe it’s just good old American overconfidence.
The tension in placebo surgery vs placebo tablets is that everyone feel less anxious about giving people a placebo tablet than doing a fake surgery. But if a surgery (or cardiac procedure) is done to improve qualitative symptoms, how else does one separate the placebo effect of having an operation?
A recent tricuspid valve clipping trial called TRILUMINATE reported positive results driven only by subjective outcomes. However, one group got a cardiac procedure and the other group got tablets only. It’s a worthless trial because there is no way to sort out placebo effect.
On the gradient of placebo effects, it’s well known that big pills (capsules) have larger placebo effects than small tablets, costlier pills have more effect than inexpensive pills. Placebo injections are stronger than pills, and, of course, placebo surgery carries the strongest placebo effect.
The medical literature is replete with major reversals in surgical procedures. Claude made me a nice list:.
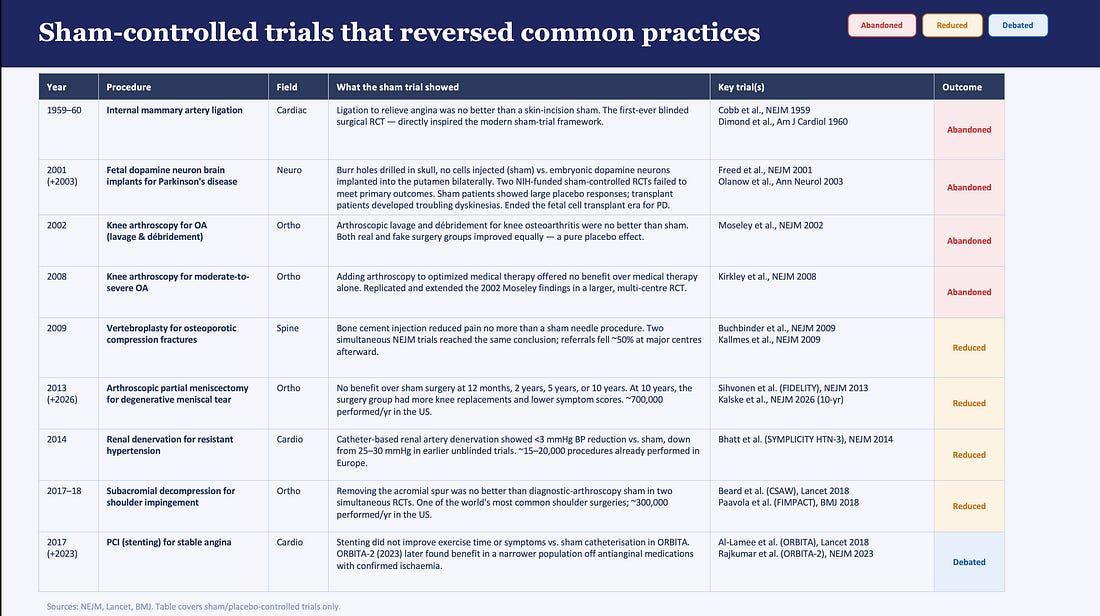
The second one in the table is especially remarkable as the placebo surgery involved drilling burr holes into the skull without injected anything. Turns out the trial was negative and the highly invasive surgery was abandoned.
The ethics of placebo trials
People always ask about the ethics of placebo surgery. To me, it’s a simple question. You must balance the ethics of exposing a hundred or so people to a placebo surgery vs hundreds of thousands to a useless or potentially harmful surgery. The former seems wiser than the latter.
Let me know what you think. And thanks for being part of Sensible Medicine
You’re currently a free subscriber to Sensible Medicine. For the full experience, upgrade your subscription.




Leave a Reply
You must be logged in to post a comment.