Systemic Treatments for the Cell Danger Response (CDR)
July 8 | Posted by mrossol | Coronavirus, Health, MedicineSource: Systemic Treatments for the Cell Danger Response
|
|
|
||||||||||||
Story at a Glance:
•In the first part of this series, I discussed the Cell Danger Response (CDR), a mechanism cells rely upon to survive potentially lethal environmental threats.
•In the second part of this series, I discussed how regenerative medicine restores non-functional tissue and how targeted injections can rescue cells trapped in the CDR.
•In this final part of the series, I will discuss the therapies that can be used to systemically resolve the CDR, some of which we have seen offer significant improvement to individuals with spike protein injuries. Many of these were developed from regenerative medicine techniques designed to restore non-healing tissue (e.g., from an injury) and tissue that loses its function or disappears because it can no longer enter its growth phase (e.g., this causes hair loss).
The CDR is initiated by the mitochondria, who, after sensing danger, divert the cell’s resources from promoting the normal function of the cell to creating a low-functioning cell that is more capable of neutralizing microbial threats (e.g., viruses) and surviving otherwise lethal stressors. Once the CDR is triggered, cells warn the surrounding cells to enter the CDR but otherwise prioritize their individual survival and become disconnected from the tissue and organism they belong to.
Note: this disconnection causes cells to partially stop responding to a wide range of hormones (e.g., thyroid hormone or insulin) and signals from nerves (which can be quantified through abnormal changes in things controlled by the nervous system, such as the heart rate and its variability).
Two ways thus emerge to look at the CDR. The first is that it is a remarkable adaptation that makes life possible by protecting and healing cells from each injury they encounter (which is why the leading CDR researcher Nauviaux now refers to it as the healing cycle). The other is that it is the disastrous root cause of chronic illness worldwide. The critical distinction between these two is that in health, the CDR cycle can complete itself (thereby exiting the CDR), while in disease, something goes wrong, and it can’t, trapping patients in an endless cycle of mitochondrial “dysfunction.”
In our modern world, we are exposed to a massive number of environmental stressors we never evolved to handle (e.g., numerous harmful chemicals which are each present in “sub-toxic” amounts), and as a result, in many patients eventually reach a tipping point from those collective stressors where the CDR flips to becoming chronically activated and creates symptoms arising from the specific tissue where the CDR activated. This, in turn, describes precisely what transpires in many complex illnesses the medical profession struggles to address or even understand.
My focus has been drawn back to the CDR because I gradually realized it was a key issue in many of the patients with spike protein injuries, and much of what I and my colleagues saw mirrored our experiences from working with other complex patients trapped in the CDR.
Naviaux has likewise reached a similar conclusion:
Evidence is emerging that patients with long-COVID, also known as post-acute sequelae of SARS-CoV-2 infection (PASC), do not have a generalized defect in mitochondria. Instead of a generalized defect, long-COVID is associated with entry into a specifically altered state of [hypometabolic] mitochondria function. The evidence for this comes from [simultaneously measuring all of the metabolites that reflect the current metabolic function of the body].
In the case of [hypometabolic survival states like] chronic fatigue syndrome (ME/CFS), long-COVID, and related [metabolic states], bouts of physical and emotional stress can lead to setbacks called ‘crashes’ and post-exertional malaise that result from a transient shift from Phase 3A to more glycolytic metabolism and inflammation in Phase 1C of the healing cycle caused by autonomic and neuroendocrine activation.
Mitochondrial hyperfusion leads to hypersensitivity to ATP signaling, abnormalities in innate immunity, neutrophil and natural killer cell dysfunction, neurologic symptoms, latent DNA virus reactivation, endogenous retrovirus activation, misfolded protein aggregates, and a predisposition to apoptosis, ferroptosis, and other cell death pathways. Restoration of long-distance brain-body signal transduction at the end of Phase 3 of the Healing Cycle [reduces purinergic signaling]…and enables normal organ function to return, and marks the re-entry to Health Cycle.
Since there is a massive number of people with spike protein injuries (e.g., there are tens of millions of COVID survivors left with chronic fatigue syndrome and other disabilities, of whom 10–30% are unlikely to recover with the currently existing therapies), Naviaux has done a lot of work to bring attention to this issue.
The Healing Cycle
Once something triggers the CDR, the following phases should occur:
•CDR1: An inflammatory phase where the cell seals itself off and eliminates microbial invaders. A sustained CDR1 creates chronic inflammatory disorders.
•CDR2: A proliferative phase where missing cellular components and cells are replaced (e.g., via making new blood vessels, new cells, and recruiting stem cells). A sustained CDR2 can create chronic proliferative disorders like cancer.
•CDR3: An anti-inflammatory, reintegration, and differentiation phase where the cell becomes able to resume its normal function and reconnect with the rest of the body. A sustained CDR3 can lead to various complex disorders (e.g., neurodevelopmental, affective, neuropsychiatric, or neurodegenerative). When CDR3 completes, the cells and tissues are frequently healthier than they were before initiating the CDR—a fundamental principle regenerative medicine utilizes to restore lost functionality.
The healing cycle is initially sustained by the cells signaling danger to each other (and later the body) with ATP, then is terminated by safety signals from the entire body (e.g., via the vagus nerve). This termination requires CDR3 to re-establish the cell’s communication with the body and for the individual to exist in a “safe” environment that produces safety signals for the body. Conversely, if the initial threat that triggered the CDR has not been eliminated, the body evolved not to send signals to terminate the CDR. This is a key reason why the long-lasting synthetic mRNA (which continually produces the toxic spike protein) is so problematic.
Note: In addition to getting stuck along the progression of CDR1 → CDR2 → CDR3 → normal cell function, cells can also be shunted into the hypometabolic survival state mentioned above (e.g., this happens in chronic spike protein injuries, CFS, or chronic Lyme disease). Typically, for the first 3-6 months, the mitochondria that have switched to sustain the CDR can easily switch back to their normal function. If the CDR persists past this point (which frequently happens in these illnesses), the mitochondria become much more challenging to switch back, and pathological structural changes develop in organs and tissues.
This model both explains why so many different things can trigger the “same” complex chronic illness (as in each individual their confluence of stressors met the threshold for starting a sustained CDR) and why so many different “healthy” practices (e.g., numerous supplements, stress reduction or good sleep) can partially improve but not resolve these illnesses. Furthermore, as discussed in the previous article, to varying extents, everyone has impaired tissue and organ function from cells trapped within the CDR, and this issue worsening is one of the key causes of the loss of function seen with aging.
Since this muli-factorial model is so outside our traditional one cause one effect model of medicine, it is somewhat understandable many of these complex conditions are cruelly labeled as being “psychosomatic” (in the patient’s head). This problem is further worsened both by the fact the CDR often creates depression or anxiety, while negative emotions cause the brain to signal danger (which worsens the CDR), which in turn prevents the patient from embodying positive emotions that signal safety and resolve the CDR.
Rebooting The Healing Cycle
To treat the CDR, Naviaux advocates for a relatively straightforward approach. Replacing things that signal danger with those that signal health (which he terms salugenesis) and directly blocking the signals for the CDR. According to Naviaux:
The six cardinal elements of the health cycle are 1) wakeful activity, 2) nutrient intake, 3) waste and toxin removal, 4) social connection [and positive social support], 5) nature connection, and 6) restorative sleep. Absence of, or abnormalities in, any of the cardinal elements of the health cycle can lead to pluricausal disease [while] their presence contributes to the building of functional reserve capacity and resilient health over the weeks and months after injury or illness.
While his six points are relatively simple, they also touch upon a critical issue. Medicine typically focuses on identifying and “treating” diseases rather than identifying what creates health and cultivating that. Although the disease-focused model can often seem very impressive (and generate a lot of business from each identified “disease”), without cultivating the core generators of health, complex chronic diseases will continually arise that cannot be fixed within the disease-centered model.
Diving into the technicalities, I believe some of the most important things for anyone seeking to facilitate the health cycle are as follows:
•Restore a healthy balance between the rest and relaxation (parasympathetic) and the fight or flight (sympathetic) branches of the nervous system—Excitatory circuits trigger the CDR and anxiety, while inhibitory circuits are used for calming and safety signaling. This is a crucial part of why stress reduction and positive emotions can be quite helpful for CDR illnesses. Unfortunately, CDR patients are frequently stuck in a state of chronic sympathetic over-activation and parasympathetic deficiency.
Note: the vagal (parasympathetic) nerve travels all throughout the body. It is filled with ATP receptors it uses to detect the CDR in any tissue and then alert the body to a danger present, leading to it being called “the great wanderer and protector.”
•Restore normal sleep architecture (e.g., deep sleep), as this period is used by the nervous system to signal safety to the body (delta waves play a crucial role here)—Unfortunately, an active CDR disrupts normal sleep patterns. Over the decades, countless integrative practitioners have consistently observed that restoring healthy sleep is vital for chronically ill patients but, unfortunately, often quite challenging to restore.
Note: the most effective methods I have found for healing the sleep cycle are discussed here. One of the most important things to understand is that most “sleep” medications are neurological sedatives that inhibit the brain’s ability to enter the restorative phases of sleep.
Additionally, one of the primary molecules that signals sleepiness to the body, adenosine, is a product of ATP being broken down by regular metabolic activity throughout the day. Caffeine, for example, keeps you awake by blocking the adenosine receptors in the brain. In many individuals, that effect can persist for hours after consuming it (which is one of the many things that may need to be addressed when teaching insomnia).
Conversely, adenosine counteracts some of the effects of the CDR, and I have wondered if one of my favorite herbs (which works by activating adenosine receptors) could also be used to counteract the CDR (the herb is well known for effectively treating both insomnia and chronic pain, and inconsistently helping with anxiety). I have wondered if this herb could also help with the CDR.
•Restore the normal rhythms of the body (e.g., the circadian rhythm)—This concept is now relatively understood for the sleep cycle, and many leaders in the integrative medical field strongly advocate avoiding exposure to signals that disrupt the normal timing of the sleep cycle (such as blue light at night). However, sleep is not the only rhythm disrupted by modern technology.
Quite a few of my most knowledgeable mentors (I immensely trust their judgment) have long believed one of the primary causes of the massive loss of vitality and rise in chronic illness we’ve seen over the last 150 years is due to modern technology disrupting many of the rhythms the body depends upon to regulate itself. Some of these include temperature (hot during the day, cold at night), moving or remaining sedentary, and appropriately pacing the output of the nervous system (e.g., not making more than seven decisions in a row before having a rest period—something almost impossible to achieve in the computer age). Now and then, I hear stories of people returning to a primitive lifestyle (e.g., one patient with a wood stove used no electricity or gas during a cold winter) and having considerable improvements in health from being forced to follow the natural rhythms of the environment.
Note: Nauviaux touches upon another important point relating to these rhythms—the body requires pulsed rather than continuous signals to regulate itself. A frequent error individuals in the integrative medicine field make is giving something they believe is “good” for you continuously rather than in a pulsed fashion, which often can reverse the benefit of an otherwise beneficial therapy. This is also why recovering from a chronic illness typically requires “safe” periods free of external stressors and why it is so easy to reactive a CDR pattern in the fragile period after the initial recovery from a chronic illness (this is a really frustrating issue); it seems to take about three months, the length of a season, to solidify a new pattern within the body.
Nauviaux argues that since cells that entered the CDR remain in it until they receive sufficient safety signals from the body, “healing is an active process that requires positive reinforcement with non-danger, safety and security signals from the brain,” and that in many cases if an existing CDR is not addressed through salugenesis, it can create significant illness far down the road. This has been best demonstrated by the chronic diseases that result from unresolved trauma from childhood but also occurs with other adverse events (e.g., toxin exposures earlier in life). To quote Nauviaux:
If long-distance safety signals are not re-established after the initial damage from infection or injury are repaired, the tissue defaults to chronic defense at the cellular level.
Blocking the CDR
The body relies upon ATP to signal danger. This is likely due to approximately one million times as much ATP existing within the cell as outside it, so when ATP increases outside the cell, this serves as a relatively universal signal that a cell has been damaged and its contents are leaking into the surroundings. As a result, various receptors exist throughout the body for ATP and related purine compounds (termed purinergic receptors). Conversely, in addition to purines leaking out on their own, a variety of channels ATP can pass through exist in the cellular membrane, which open up when cells sense danger, thereby allowing them to signal that danger to their environment.
Presently, one drug, suramin (an antiparasitic medication for African sleeping sickness) exists that blocks all of the purinergic receptors throughout the body. In addition to suramin, other drugs that block specific purinergic receptors exist, many of which have been demonstrated to improve autoimmune disorders Nauviaux associates with the CDR:
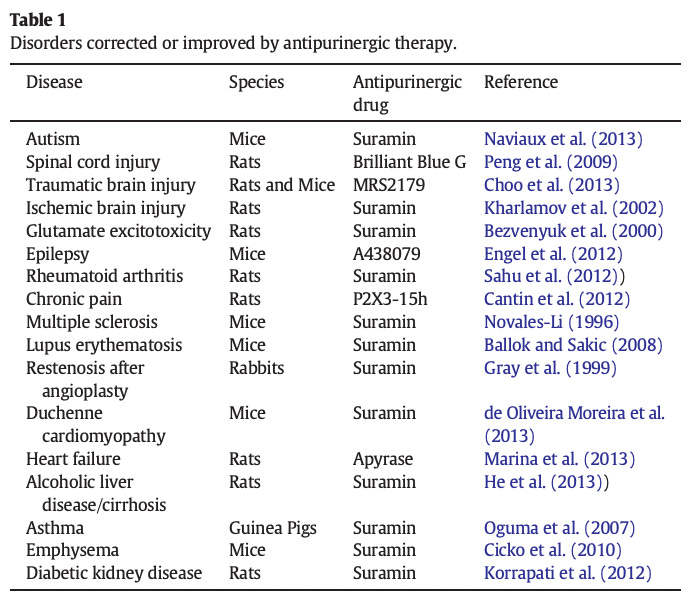 |
In addition to the above:
•Brilliant Blue G has been found to help with Parkinson’s disease and acetaminophen-associated liver injury.
•Suramin protects against Fas-induced acute fulminant hepatitis in mouse models •Purinergic signaling was recently shown to play a vital role in inflammatory bowel diseases—a targeted anti-purinergic drug (APD) both reduced the inflammation present in mice and improved their response to conventional therapy.
•Several experimental APDs are in clinical trials for rheumatoid arthritis and pain that target the P2X7 receptor.
Note: ATP signaling also potentiates pain and heat sensory perception. This is why treating the CDR can often improve chronic pain and may explain why patients with complex illnesses are hypersensitive to certain stimuli (an alternative explanation is that they suffered zeta potential collapses that triggered microstrokes in the thalamus, the part of the brain responsible for dampening pain signals from the body).
One of the most intriguing uses of APD therapy is for mast cells, which assist in the immune response by degranulating and releasing histamine (one of the biomolecules most commonly associated with allergies and one that elevates during CDR1). Extracellular ATP, ADP, adenosine, and UDP-glucose are essential regulators of mast cell degranulation, and in 2019, it was demonstrated that mast cell degranulation is inhibited by suramin.
In many complex chronic illnesses, a mast cell activation disorder develops where mast cells become prone to degranulating from very light stimuli, making patients highly sensitive to many seemingly innocuous triggers (which makes life incredibly challenging). Since mast cell disorders commonly develop in COVID-19 vaccine-injured patients, more are becoming aware of this condition.
Autism and Antipurinergic Therapy.
Autism is virtually impossible to treat (at least within the conventional paradigm), and evidence suggests it results from an unresolved CDR. For example, autism is known to improve during fevers, suggesting metabolism influences the disorder, and each of the shared genes known to increase the risk of autism can be shown to play a role in CDR signaling or maintenance.
Note: fevers occur during CDR1; autism is a CDR3 (non-fever) disorder.
Because of this, Naviaux researched treating the condition with antipurinergic therapy under the theory doing so would terminate the signal that perpetuated the CDR. The initial results in mice (this study, this study, and this study) were encouraging. For example:
In a mouse model of autism, when treatment was delayed until the human biological age-equivalent of 30years old, the core functional abnormalities in behavior and metabolism in ASD could still be completely corrected with antipurinergic therapy (APT) with suramin, but the gait abnormalities associated with the structural loss of cerebellar Purkinje cells were not reversed
Naviaux then proceeded to a pilot clinical trial which found:
This study of 10 boys, ages 5–14 years, showed that all 5 boys who received [low dose] antipurinergic therapy (APT) with a single intravenous dose of suramin experienced improvements in all the core symptoms of autism that lasted for 5–8 weeks. Language, social interaction, restricted interests, and repetitive movements all improved. Two children who were non-verbal spoke their first sentences. None of these improvements were observed in the placebo group.
Suramin treatment was synergistic with regular school, educational enrichment programs, applied behavioral analysis (ABA), speech, and occupational therapy.
Note: I think the increased responsiveness to behavioral therapies once the CDR is blocked is a very important point.
Following Naviaux’s 2017 trial, in 2018, PaxMedica (a biopharmaceutical company focused on finding treatments for unsolved neurodevelopmental disorders) was founded and attempted to replicate Naviaux’s work in South Africa.
In PaxMedica’s randomized, double-blind, placebo-controlled trial of 52 boys with moderate to severe autism, IV suramin was administered at the start of the trial, at week 4, and at week 8. The children were assessed for improvement throughout the trial (with the final assessment occurring six weeks after the 3rd dose), and significant benefit was observed in those who received suramin.
PaxMedica’s trial was supposed to be published in a peer-reviewed journal, but it ultimately was only presented at a conference (I talked to people involved with the trial who verified that it demonstrated that suramin was a viable treatment for autism). A larger follow-up trial to PaxMedica’s trial was planned but has not yet been conducted.
Note: All of these trials utilized suramin since it is still not known which of the 19 purinergic receptors are specifically responsible for sustaining the CDR, and thus a broad spectrum antipurinergic therapy (suramin being the only one available to humans) was needed to have a guaranteed effect
From doing this research, Naviaux determined low doses of suramin (5–15 μM) were sufficient to treat the CDR, suggesting this dose was relatively safe. For context:
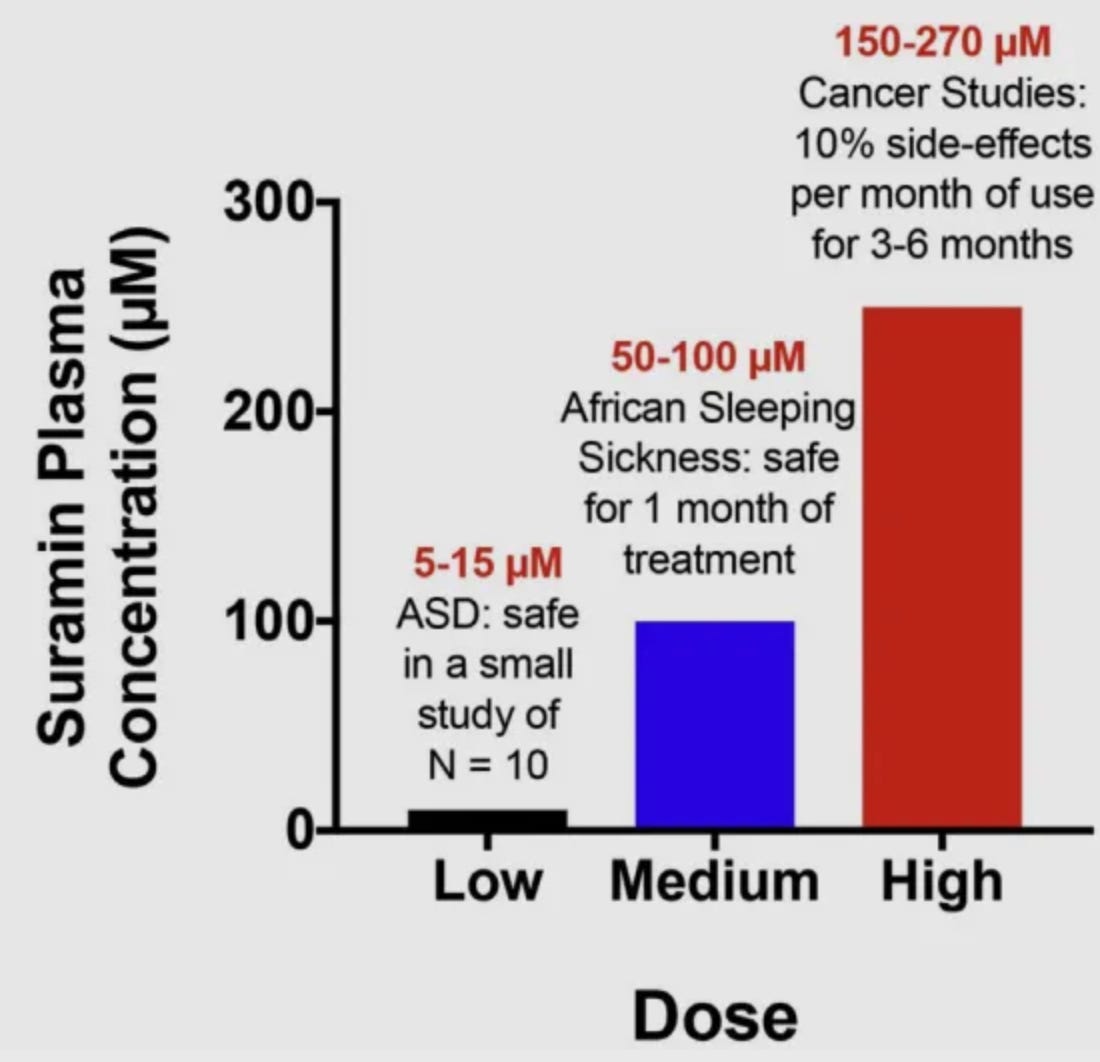 |
Naviaux’s low-dose trial monitored the subjects and their blood work for signs of an adverse reaction. The only side effect observed in the low-dose trial was a minor rash (described as an evanescent, asymptomatic, fine macular, patchy, morbilliform rash) which appeared over 1–20% of the body approximately one day after the infusion and disappeared spontaneously in 2–4 days.
In the follow-up trial in South Africa, the most common adverse effects from Suramin were rash, upper respiratory infection, and vomiting. Most of the side effects were mild to moderate in severity and resolved with no intervention. One serious adverse event occurred in a patient who received Suramin with multiple concomitant conditions that resolved without sequelae following acute treatment.
Note: earlier trials in Africa established that the half-life of Suramin is 14.7 ± 0.7 days (excluding the 10% of the subjects who metabolized it faster), signifying a lengthy duration of action from a single dose (e.g., the 5-8 weeks in the autism trial). Unfortunately, since it has not been possible to conduct any follow-up research, it is not known what benefits occur (e.g., an increased period of improvement or permanent improvements) if Suramin is given multiple times (e.g., monthly) for patients with autism. There is reason to suspect this both since the half-life of Suramin increases with multiple doses (e.g., previous research showed dividing a monthly infusion into five weekly infusions increased its half-life by 3-4 times) and because suramin administration was synergistic with behavioral therapy.
Presently, Suramin is, for all practical purposes, unavailable because the company which manufactured it (Bayer) stopped producing it a few years ago (it was only made at one facility, and that production plant was shut down as part of a transition Bayer had put into motion years before due to the economic viability of the African sleeping sickness). Since Suramin is challenging to produce correctly, there is currently no available source of Suramin (although PaxMedica has been trying to raise funds to create a new production facility).
Additionally, since the parasite which causes African sleeping sickness does not exist within the United States, it has no approved use here, and it is illegal to import Suramin into the US for human use without FDA approval. As a result, despite the work Nauviaux and others have put into addressing this issue, treatments for the CDR remain mostly unknown and almost entirely unavailable to the general public.
Note: antipurinergic activity has been identified in a variety of natural herbs that have therapeutic benefits matching their predicted antipurinergic effects (detailed in this study and this study). It is quite likely numerous botanical products will be identified in the future that also have positive effects on the CDR.
However, while neither Suramin nor any other antipurinergic drugs are available, a few other approaches to treat CDR are also being explored. For example, one of the major issues in aging is cells of the brain “turning off” due to an unresolved CDR. One of the more promising approaches to treating cognitive decline treats this by disabling what is referred to by its proponents as the “integrated stress response” (something which has many overlaps with the CDR):
“The principle that blocking protein synthesis prevents long-term memory storage was discovered many years ago. With age there is a marked decline of protein synthesis in the brain that correlates with defects in proper protein folding. Accumulation of misfolded proteins can activate the integrated stress response (ISR), an evolutionary conserved pathway that decreases protein synthesis. In this way, the ISR may have a causative role in age-related cognitive decline.”
When tested, an ISR inhibitor was found to restore the structure and function of cells within the brain and to improve a variety of age-related memory deficits.
Note: For numerous reasons (e.g., its many parallels to AZT, the toxic AIDS drug Fauci pushed on the market), I was very concerned about remdesivir after it was arbitrarily chosen to be the standard of care for COVID-19. From the start, I suspected remdesivir (which works by inhibiting viral RNA polymerase) might also affect human RNA polymerase and partially inhibit human protein synthesis.
Since then, we’ve had a few patients who survived a course of remdesivir and then received prolotherapy after being discharged from the hospital. In those patients, prolotherapy (which, as discussed in the previous article, uses an irritating stimulus to initiate the tissue repair process) does not work for a few months. We assumed this was due to remdesivir blocking the regenerative effects of prolotherapy (e.g., by blocking protein synthesis) until it cleared from the body. However, it could have also been the result of a subtle but sustained systemic CDR arising from a severe COVID infection.
Working with the CDR in Clinical Practice
One of my colleagues has decades of experience working with challenging patients whose illnesses are beyond the ability of most integrative medical practitioners to treat. My colleague was drawn to the CDR since it explained why patients responded so poorly to many therapies that “should have” worked, and over time reached the conclusion the CDR was at the root of many of the illnesses they saw in their clinic.
I thus was very interested to hear their perspectives on treating the CDR. They told me that the CDR is a helpful story for understanding the complex illnesses you see, but it’s not the magic bullet everyone hopes for. This is because there is no one signal (with the possible exception of suramin—which no one can obtain) that reverses the CDR’s inflammation and causes cells to go from CDR1 to CDR2 to CDR3 to normal and resume communicating with the body.
They also felt the CDR was very useful in helping one to understand which therapies to avoid and to recognize that many of the things you think you “need” to treat are just physiologic compensations that should be left alone. Generally, the CDR model was the most helpful if you focused on one specific system of the body and how to switch it back to normal (which is partly due to a lack of available therapies that globally improve the CDR). Since the CDR is constantly happening throughout your body at different times and levels, it is critical to be clear on what cells you are talking about when one decides to “treat the CDR.”
Some of their key insights from years of working with the CDR were:
•Suramin seems to transiently stop the CDR for about two weeks, at which point the CDR resumes unless the underlying factor triggering it is addressed. Since the CDR can often result from a danger long since passed (e.g., years ago) or a currently active one, untangling what to do can become very confusing.
Note: I believe this also explains why our preferred treatment for CDRs caused by spike protein injuries often permanently fixes long covid after one administration, whereas mRNA vaccine injuries require numerous administrations.
•The order of treating a CDR superimposed with an active danger (e.g., an infection) is complicated. If people have too many feedback loops, you can’t target the pathogen initially because it will significantly exacerbate their CDR. Likewise, many things that seem restorative or cleansing to the body can often heavily backfire in CDR patients due to additional signals each intervention creates in the body. Furthermore, CDRs often become more and more sensitive to additional triggers as the disease progresses. For these reasons, in patients with an active CDR, I and many others try to avoid anything we suspect might create too fast of a shift in their system. However, despite this caution, I still have had numerous cases I provided a low dose of a therapy I thought the patient needed to get to the next stage of healing, and instead of it helping the patient, it signals their body to jump back into the CDR.
To provide a simplified version of the process for these patients, typically, you have to either:
-Treat the CDR (this is often correct if the danger is long gone).
-Treat the active danger, then treat the CDR.
-Treat the CDR, the active danger, and then the CDR again.
Additionally, detoxification is often necessary to perform before any of these (and sometimes before that, a much lighter form my colleague termed “pretox”), as are therapies that improve the existing fluid circulation (e.g., by improving the existing zeta potential). This is because poor circulation to cells can be a trigger for the CDR, and any toxin shift requires a working circulation to drain the fluids so they do not build up and concentrate in a specific area (this encapsulates why giving antibiotics to a patient with Lyme disease who has an impaired fluid circulation can be so problematic).
It is thus critical to recognize that while many therapeutic approaches can improve symptoms resulting from the CDR, it is critical to determine if your therapy temporarily dampened a patient’s CDR or shifted their body to a new state of health.
•The end organ signaling resistance to hormones and other growth factors created by the CDR is very important to be aware of. In addition to signaling therapies (e.g., thyroid supplementation) being ineffective, since there is a mix of responsive cells (those not in the CDR) and unresponsive cells in the CDR, those therapies can often create a dependence (e.g., insulin in diabetes).
Note: in these situations, some of my colleagues find using low doses of T3 (Cytomel) in the range of 2.5 mg rather than regular doses of T4 (Synthroid) helpful. Also, in addition to normal thyroid labs, it is often necessary to test for reverse T3 to guide one’s treatment.
Furthermore, they will over-activate the body and create a variety of complications (e.g., iatrogenic side effects), many of which result from the still functional tissue being over-activated or the CDR’d tissue being activated when it was not ready to be activated. This is also what often happens if one attempts to increase poor mitochondrial function with supplementation rather than treating the CDR (which is reducing mitochondrial function as part of a normal adaptive response).
Note: Nauviax argues this also frequently causes complex endocrine syndromes (e.g., thyroid or adrenal exhaustion syndromes) that do not fit classical medical definitions of deficiency or failure because residual hormone production can usually be shown by physiologic stimulation but is otherwise suppressed.
•Nauviax’s concept of salugenesis is frequently helpful but often not sufficient to treat the CDR.
•Fasting (intermittent and long-term) somewhat helps turn down the CDR since a fasting metabolism reduces excessive immunological activity and inflammation. Fasting will trigger the body to eliminate sick cells (which are often trapped in the CDR and disrupting the rest of the tissue) through autophagy, but normally won’t eliminate all of them.
Note: in a recent series, I shared my perspectives on the various diets out there and the most effective approaches I know of for losing weight—a condition which, like the myriad of CDR illnesses, I believe is a product of incorrect signaling throughout the body. Furthermore, it can also be argued obesity is partly a product of the hormonal resistance created by the CDR.
One of the great questions in this area is whether the ketogenic diet is or is not good for you (as there is evidence supporting both interpretations). In a recent study that tested the effects of injected ATP (which triggers the CDR) on mice, activating the CDR caused cells to switch from a balanced usage of carbohydrates to nearly complete dependence on fatty acids. This suggests that conditions that respond well to ketogenic diets (particularly ones in the central nervous system, such as epilepsy) respond because the diet provides nourishment to cells trapped in the CDR. Conversely, it also suggests that the ketogenic diet is not what the body wants in normal health.
•My colleagues strongly agrees with this perspective shared by Nauviax:
Antipurinergic drugs like suramin, pannexin 1 (PANX1) channel blockers, and other salugenesis therapies are part of induction therapy to reboot healing. They are not meant to be taken for life. These interventions are meant to be bridges. During the induction phase, interventions are meant to act like a cast for a broken leg—they are intended to support the healing process and protect injured tissues from further damage. Once the healing cycle is completed and reentry into the health cycle occurs, then antipurinergic therapy can be discontinued.
Regenerative Medical Treatments of the CDR
As discussed in the previous article, regenerative medicine restores functionality to tissue either by:
•Replacing lost tissue with new tissue (e.g., by using stem cells).
•Reactivating dormant tissue by restoring non-functional and non-dividing cells.
Much of regenerative medicine, in turn, comes down to figuring out which is occurring and how to address it. Since the latter (dormant tissue) is more frequently the issue, regenerative medicine has discovered a variety of highly effective treatments for reactivating those cells—which is extremely helpful for the subject at hand as the CDR causes cells to become dormant.
In many cases, the underlying issue for a patient is specific groups of cells that have become trapped in the CDR, causing either a local effect (which the patient typically can identify) or a systemic one (which is more difficult to trace back to the group of dysfunctional tissue). For example, following surgery, incomplete healing of the cut tissue leads to a chronically activated CDR there. This can cause discomfort within the scar, but it can also activate the central nervous system creating a wide array of systemic complications that can “miraculously” improve or resolve following treatment of the scar.
Once a danger activates a CDR, the sensitivity of cells trapped in that state to additional dangers increases. Since the spike protein not only creates a significant danger but remains in place for a prolonged period (as the vaccine mRNA was designed to resist degradation in the body), it causes existing CDRs to significantly worsen (best shown by the inflammatory flares frequently associated with the vaccine). This results in injuries like old dormant scars developing into a searing pain, and I’ve seen numerous cases where significant improvement to vaccine injured resulted from using neural therapy to treat an old scar.
However, while local treatments of dormant tissue are sometimes helpful, in many cases (e.g., when the vaccine spike protein triggers the CDR throughout the body) a systemic regenerative therapy is needed instead.
Systemic Regenerative Therapies
In a previous series on Alzheimer’s disease, I discussed the catastrophic costs of the disease to society, the century of corrupt and misguided research into it (which has focused on treating a protective adaptation rather than a cause of the disease), and the fact that effective, and clinically proven (but non-commercializable) treatments have been developed the multibillion-dollar Alzheimer’s research industry won’t even acknowledge. Because of this dysfunctional paradigm, we are now seeing dangerous and non-effective Alzheimer’s drugs be pushed onto the market, which the FDA’s leadership is working directly with the pharmaceutical industry to promote to the public.
Alzheimer’s disease is essentially a result of brain cells becoming deactivated and, eventually, being eliminated during the brain’s natural remodeling process. In turn, treating Alzheimer’s becomes a process of:
•Reducing the shocks to those brain cells that cause the dormancy (inhaled anesthetics used in surgery to “temporarily” turn off neurons are one of the most common triggers, but many other toxins may also need to be addressed).
•Providing sustained nourishment to the cells (e.g., nutritionally, through active cognitive activity, or by restoring their proper circulation to the brain).
•Having the brain exit its dormancy. Sometimes this is done with nutritional support (e.g., subcutaneous aluminum-free B1 and B12 injections to support the Kreb’s cycle are very helpful, especially before and after surgery). In many cases, treating Alzheimer’s disease requires mitigating the CDR in the brain. One of our favorite approaches for treating lost neurological function (e.g., after a stroke) is with DMSO, which can revive cells that have not been too severely affected by the CDR.
Note: the common form of hair loss is “Telogen Effluvium.” This name is based on the fact hair cycles through three phases, a growth phase (anagen), a pruning phase (catagen), and a resting phase (telogen). If hair spends too much time in the resting (telogen) phase, hair gradually becomes lost. While they were not initially developed to deal with hair loss, all of the most effective approaches I’ve seen for treating hair loss are regenerative therapies (discussed below) which essentially bring cells out of their rest phase and back into their growth phase.
I’ve wanted to write about the approaches the regenerative medical field uses to systemically treat the CDR, partly because it becomes more and more important as you age (due to cells having increasing difficulty exiting the CDR) and partly because it’s often crucial for addressing long COVID and vaccine injuries.
However, I’ve held off on doing so partly because I wanted to provide the necessary context beforehand (this series took me over a hundred hours to put together, so it took a while to finish) and because I did not want to create accessibility issues for those already relying upon these therapies to treat their vaccine injuries. Because of this, the second half of the article will need to be reserved for a more limited audience…
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.




Leave a Reply
You must be logged in to post a comment.